Around the world, there is reason to hope. Here are some examples of nations who have either controlled, or are starting to see huge regression of rates of COVID and hospitalisation.
The key is
-
They ALL have over 90% of their eligible population vaccinated.
-
They all test their populations and maintain excellent Contact Tracing, and have a population that abides by restrictions to people who test positive, or have symptoms.
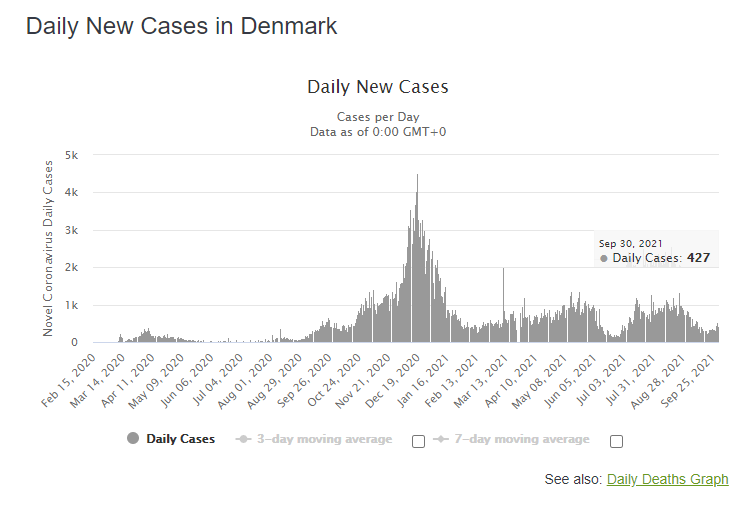
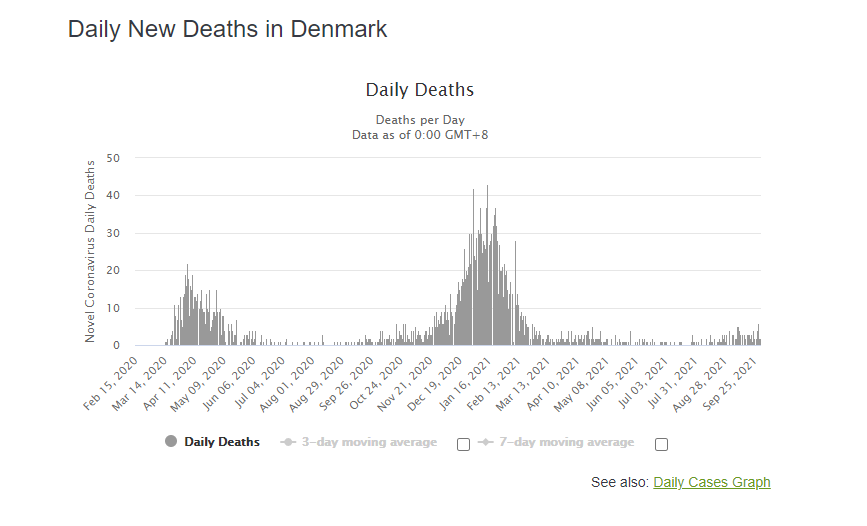
Denmark –
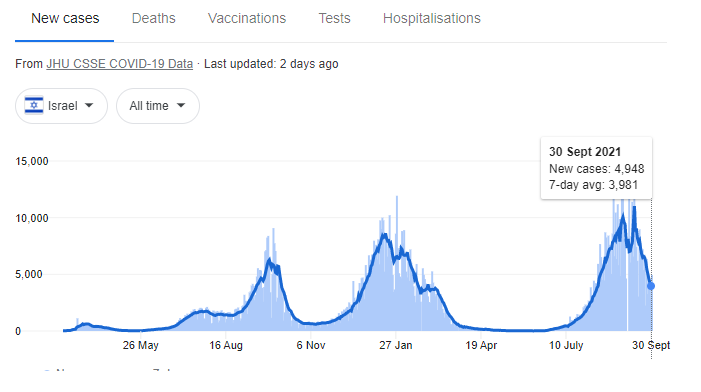
Israel
Portugal

The UK
The UK has had 82% of its population double vaccinated. Yet vaccination uptake has stagnated. Unfortunately, a lot of misinformation spreads there, similar to the US. Currently, they are 130-135 deaths per day. By comparison, that would be equivalent to Australia seeing 48 deaths per day, which is almost 5x higher than what we’re seeing on average here. It’s important to know that they have almost 15x more cases per day there. So a higher vaccination rate DOES work in reducing hospitalisations. But sadly, their hospitals are quite strained – with over double the ICU bed usage (adjusted for the UK’s larger population). They did also use a different vaccine – but one shown to have similar efficacy in reducing hospitalisation and severe death against the delta strain (in any case, we in Australia also used the AstraZeneca vaccine). This is why we need a HIGHER vaccination rate than 82%!

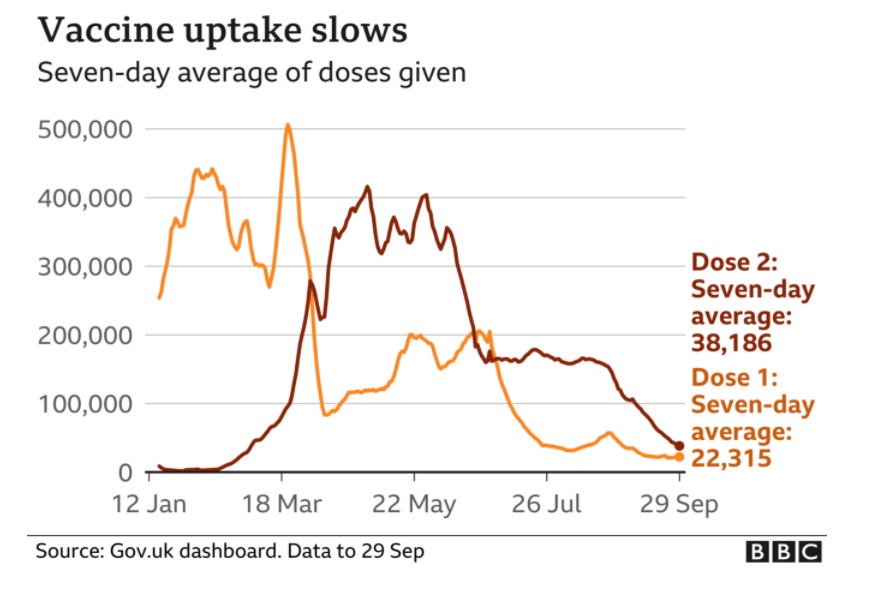
There is reason for alarm. And this is likely why cases, deaths, and hospital strain is not going down there. I have friends in healthcare there who are struggling to keep up. I hope this trend doesn’t continue.
Iceland
Iceland has controlled the delta Virus, without lockdowns, or restrictions of any kind, at any point. They did this through mass testing and effective and comprehensive contact tracing. I discuss this in detail, and how we can use rapid antigen test screening to mitigate this. At the very least though, targeted, regular rapid antigen tests, in addition to regular PCR testing for symptomatic or exposed populations may reduce the likelihood of COVID-19 outbreaks. And we NEED to emphasise this. I feel like in NSW, we’re losing focus of this as Lockdown fatigue affects us all. Find out more on Iceland’s contact tracing strategy too.

Iceland is a great example of how mass testing and contact tracing alone works! But with a vaccination rate of >95% likely responsible for reduction in transmission, a shining example of how high vaccination helps too.
As usual with all my posts – all sources are linked here. I don’t have enough time to reference them all – but all science claims are backed up by relevant peer reviewed sources.

But there is a way we can break free of this. And we NEED to give it a shot.
There’s a country that’s beaten COVID back, numerous times – even before the vaccine – and even after the Delta strain, WITHOUT LOCKING DOWN. They didn’t even close borders. And they’ve controlled a surge of the delta strain (it surged despite >80% of the adult population being vaccinated) with this strategy.
Well there is. What country is that? Iceland.
So how is Iceland, the country antivaxers said was proof vaccinations don’t work, beating COVID/doing this?
Watch this video to find out how, and keep on reading to see EXACTLY how we could do this in NSW.
By testing everyone. Even asymptomatic people.
And then getting people to isolate, not just people and their households, but close contacts too for a full 14 days, and following up on them. Regularly.
Why does this work? Well, the thing that’s made COVID dangerous is the fact that you can spread it for a long time while asymptomatic. The delta strain is worse. This Nature lay person summary breaks down why well. You start detecting the delta strain 4 days after exposure, versus 6 for other strains, and you have 1200 more viral particles than other strains too, meaning you’re more infectious, and more likely to spread it, for longer.
A lot of the time, you’ll still be asymptomatic during this. You won’t even know you’re spreading it. Which is why the delta strain’s R0 – a measure of its transmissibility – is 2 – 4x higher than previous strains.
This probably makes testing asymptomatic people even more important.
Yet our health minister wants to stop people from getting tested. Probably because the time to getting test results back is getting too high (this, at least, is reasonable).
So how can we do what Iceland did, despite having 20x more people?
By doing something no-one else is, yet. Rapid antigen test screening.
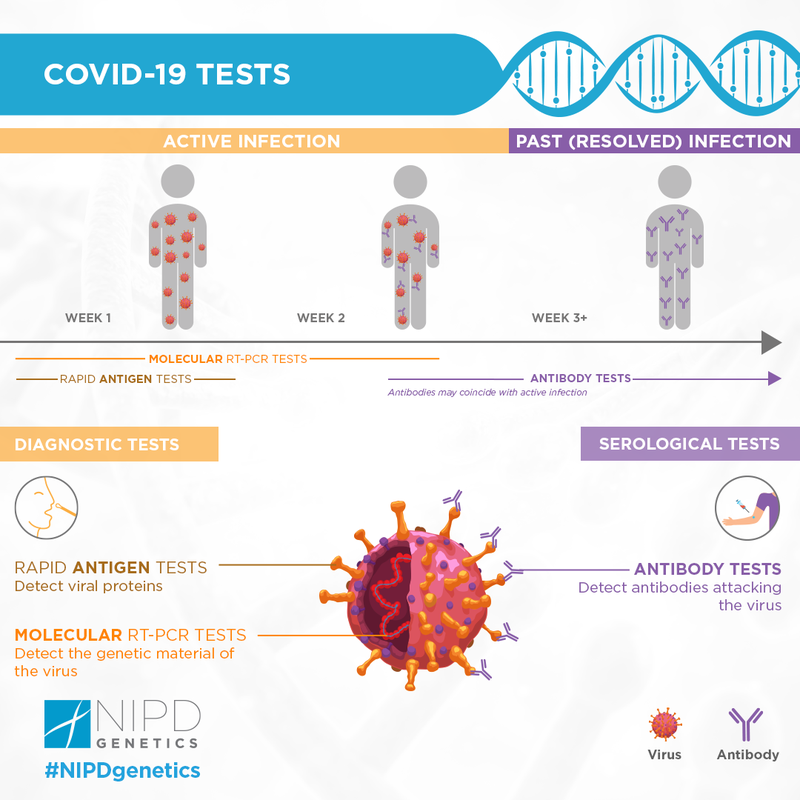
Rapid antigen tests aren’t as sensitive, but they’re cheap, can be used to test more people, more regularly, and perhaps our best way out!
PCR testing measured by labs is resource intensive. And it costs a lot too. Sydney spent over half a billion on PCR tests in the first month of the pandemic. It’s been a month since and testing has gone up MORE.
Labs earn between 60 and 120 dollars per test.
A rapid antigen test costs $5-10. Even though NSW requires healthcare staff do this, currently, other nations sell these over the counter, and are doing them at home.
Yes, they’re less sensitive meaning you’ll miss more cases (they accurately pick up 72% of symptompatic cases, and 58% of asympomatic cases),
But first off – you’ll be able to test 10, 20, maybe 30x more people at the same cost. Statistically speaking, you’re DEFINITELY – 100% – gonna pick up more cases if you screen this many more poeple!
And secondly – it was found that if you repeated these tests every 3 days, the sensitivity rose to over 90% mitigating its lower accuracy.
We do need highly accurate PCR tests for sure. But save these for people who had huge exposure, their household members and people who work in hospitals.
Give out everyone who needs to work, people in high risk areas, and more these tests, and then have them confirm this with a PCR, and we’re half way there.
This is VITAL. Not only has this been shown to work in Iceland, in real time (it’s even working against the Delta strain), we know that asymptomatic people comprise a large proportion of actual COVID cases –43%, in previous strains (which were less transmissable).
The next step – follow up with them REGULARLY. Call people up. Make sure they’re at home, and get close contacts to stay home and remind them to stay home too. Yes, that’s a lot of effort. But first off – we KNOW this works. It didn’t just work in Iceland. Early on in the pandemic, Italy tested 3300 people, found out 43% of cases were asymptomatic, and got these people, in addition to the symptomatic population to stay home. This is what stopped COVID-19 in its tracks.
Right now, it seems hard to do this in Sydney, a population of 6million people – 10x more than Iceland. But we have 21000 active cases. If you dedicated 100 of our troops (recently 500 soldiers were recruited to help this) to this, calling people up every 3 or 4 days, that’s only 20 calls a day. I did that every 2 hours when calling people for my startup! Target inspections and house calls to those not picking up, you’ll also save money and resources doing this.
We spent $580million on rapid antigen tests in the first month of lockdowns in Medicare costs alone. We’re over 2 months in now and we’ve tested 3x more people.
We spent at least $30million per day doing PCR tests.
We could do 2million screening rapid antigen tests per day, and still do over 50,000 PCR tests on those who are symptomatic, who’ve been exposed recently and for frontline workers, and SAVE money! That’s enough to screen EVERY SINGLE PERSON IN SYDNEY every 3 days!
From this, we’d
NSW Health doesn’t release or capture data on how long people were asympomatic before becoming positive [you can estimate that info by looking at where random cases may have picked it up, this may be why we’re seeing so many people active in the community.
It’s not their fault all time. Many may never have known they were infected!
Almost 4 weeks ago, they were talking about rapid antigen tests. They’re already approved. It could be a lot of logistical work. But we could use an honesty system – there are low rates of people actually going out after they’ve known they have COVID – or implement an application which allows us to capture this. The NSW Government is working on an app to do this. Why not include rapid antigen tests as a part of this to at least give us this option?
If you’ve reached this point, share this with people. The more people who know about this the better. Unfortunately, noone listens to me haha. But share the video too and hopefully we can get this out there.
I’m not a public health expert (though I have some relevant qualifications in this space and have done public health as part of my medical degree). But I’m not saying we should rely on rapid antigen tests either. We need regular old, highly reliable PCR tests too. The key to Iceland’s success is they also follow up on people.
The only restrictions they’ve imposed happened very recently – to outside travellers. This strategy worked so well for them, they literally had open borders and beat back COVID every time!
I dunno about you – but I wanna fish sooner. I wanna go back to med school, knowing I’m a little bit more safe, I’m sure you wanna work too. This is a hypothesis, but something we should consider at least! Comment your thoughts below. And subscribe to my email lists to get updates on this and to keep learning.
]]>As usual with all my posts – all sources are linked here. I don’t have enough time to reference them all – but all science claims are backed up by relevant peer reviewed sources.
But what if I told you there’s a country that’s beaten covid back, many times, even before the vaccine, consistently without lockdowns. They didn’t even close borders. And they’re doing this with the delta strain too.
Well there is. What country is that? Iceland.
So how is Iceland, the country antivaxers said was proof vaccinations don’t work, beating COVID/doing this?
Watch this video to find out how, or keep on reading.
By testing everyone. Even asymptomatic people.
And then getting people to isolate, not just people and their households, but close contacts too for a full 14 days, and following up on them. Regularly.
Why does this work? Well, the thing that’s made COVID dangerous is the fact that you can spread it for a long time while asymptomatic. The delta strain is worse. This Nature lay person summary breaks down why well. You start detecting it at 4 days, versus 6 for other strains, and you have 1200 more viral particles than other strains too, meaning you’re more infectious, and more likely to spread it, for longer.
This probably makes testing asymptomatic people even more important.
Yet our health minister wants to stop people from getting tested. Probably because the time to getting test results back is getting too high (which is reasonable).
So how can we do what Iceland did, despite having a much larger population?
By doing something no-one else is, yet. Rapid antigen testing.
Rapid antigen tests aren’t as sensitive, but they’re cheap, can be used to test more people, more regularly, and perhaps our best way out!
PCR testing measured by labs is resource intensive. And it costs a lot too. Sydney spent over half a billion on PCR tests in the first month of the pandemic. It’s been a month since and testing has gone up MORE.
Labs earn between 60 and 120 dollars per test.
A rapid antigen test costs $5-10. Even though NSW requires healthcare staff do this, currently, other nations sell these over the counter. You could mail these out.
Yes, they’re less sensitive meaning you’ll miss more cases.
But you’ll be able to test 10, 20, maybe 30x more people at the same cost. Statistically speaking, you’re definitely, 100% gonna pick up more cases.
We do need highly accurate PCR tests for sure. But save these for people who had huge exposure, their household members and people who work in hospitals.
Give out everyone who needs to work, people in high risk areas, and more these tests, and then have them confirm this with a PCR, and we’re half way there.
This is VITAL. Not only has this been shown to work in Iceland, in real time (it’s even working against the Delta strain), we know that asymptomatic people comprise a large proportion of the actual COVID population.
The next – follow up with them REGULARLY. Call people up. Make sure they’re at home, and get close contacts to stay home and remind them to stay home too. Yes, that’s a lot of effort. But first off – we KNOW this works. Not just from Iceland. Early on in the pandemic, Italy tested 3300 people, found out 43% of cases were asymptomatic, and got these people, in addition to the symptomatic population to stay home. This is what stopped COVID-19 in its tracks.
Right now, it seems hard to do this in Sydney, a population of 6million people – 10x more than Iceland. But we have what, 21000 active cases? If you dedicated 200 of our troops (recently 500 soldiers were recruited to help this) to this for everyone, every 3 or 4 days, that’s only 10 calls a day. I did that every hour when calling people for my startup! Target inspections and house calls to those not picking up, you’ll also save money and resources doing this too!
NSW Health doesn’t release or capture data on how long people were asympomatic before becoming positive [you can estimate that info by looking at where random cases may have picked it up], this may be why we’re seeing so many people active in the community.
It’s not 100% their fault. They just didn’t know they were infected!
Almost 4 weeks ago, they were talking about rapid antigen tests. They’re already approved. I know it’s a lot of logistical work. But if someone got this out to people, we could still slow this down, rather than risk COVID spreading out of control.
If you’ve reached this point, share this with people. The more people who know about this the better. Unfortunately, noone listens to me haha. But share the video too and hopefully we can get this out there.
I’m not a public health expert, I have some relevant qualifications though. But I’m not saying we should rely on rapid antigen tests either. We need regular old, highly reliable PCR tests too. The key to Iceland’s success is they also follow up on people.
The only restrictions they’ve imposed happened very recently – to outside travellers. This strategy worked so well for them, they literally had open borders and beat back COVID every time!
I dunno about you – but I wanna fish sooner. I wanna go back to med school, knowing I’m a little bit more safe, I’m sure you wanna work too. This is a hypothesis, but something we should consider at least! Comment your thoughts below. And subscribe to my email lists to get updates on this and to keep learning.
]]>
The full document they put out can be accessed here. Or just scroll down. I’ll break these down point by point –
2) “The vaccine was approved early. It did not show long term efficacy.”
Yes, it was approved early, but this was due to it being an emergency. Significant data on safety had been gained prior to this, and efficacy was demonstrated to be very high through a trial with rigorous design, and COVID had killed hundreds of thousands in America alone to this point. There’s a reason this provision in FDA regulations exist. We are still collecting data on long term efficacy, but it’s been demonstrated regularly that long term immunity is formed after COVID-19 vaccination[1, 2].
https://onlinelibrary.wiley.com/doi/10.1002/cti2.1319
https://www.nature.com/articles/s41586-021-03738-2
3) “You didn’t get enough of a sample size and some age groups weren’t sampled.
So this is the thing. Vaccine studies don’t even need that many participants to get statistical power to make an apt conclusion. This study had MORE than enough (you need 10-15k to get statistically significant results typically). COVID-19 vaccine studies that led to Pfizer getting emergency approval had over 20,000. To this day, 4.5 BILLION DOSES HAVE BEEN ADMINISTERED to 31% of people in the world! This is no longer an experiment.
The fact that only 2 patients in younger groups got COVID doesn’t mean it’s statistically insignificant, it means the vaccine is very effective. You compare the numbers in both cohorts, and see how much of a reduction there is to calculate vaccine efficacy. So that part too, is wrong. In later ones they make further claims about lack of vaccine efficacy,
This study on the 2018 influenza vaccine enrolled 10,000 people. This one did 3600. That’s more than enough. If anything this had even more proof than most. It was approved for emergency use due to there not being long term data on efficacy. Safety wise, vaccines are very largely very very safe.
https://cdn.pfizer.com/pfizercom/2020-11/C4591001_Clinical_Protocol_Nov2020.pdf
https://ourworldindata.org/covid-vaccinations?country=OWID_WRL
https://clinicaltrials.gov/ct2/show/NCT00711295
https://pubmed.ncbi.nlm.nih.gov/33065035/
4) “This is NOT shown to be effective in older adults.”
You could make that argument as mainly younger patients were included in this study, but since the approval, we’ve gained a lot of data on this. 156000 patients over 70 were studied in this BMJ trial that showed 95% efficacy. This review found similarly high results.
https://www.bmj.com/content/373/bmj.n1088
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8024166/
5) Not effective in teens.
Subsequent studies on this exact age group cited as a concern by this group of ‘physicians,’ (12 – 15 year olds) show very high efficacy of 100%.
This is not being seen now as we see many younger patients being infected with the delta variant. 30-40 year olds have 4x higher risks of death compared to 18 year olds. This is affecting more young people, likely because vaccination rates are not as high in these populations. And the delta strain seems to be more dangerous. So vaccinate!
https://www.bmj.com/content/373/bmj.n881
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html
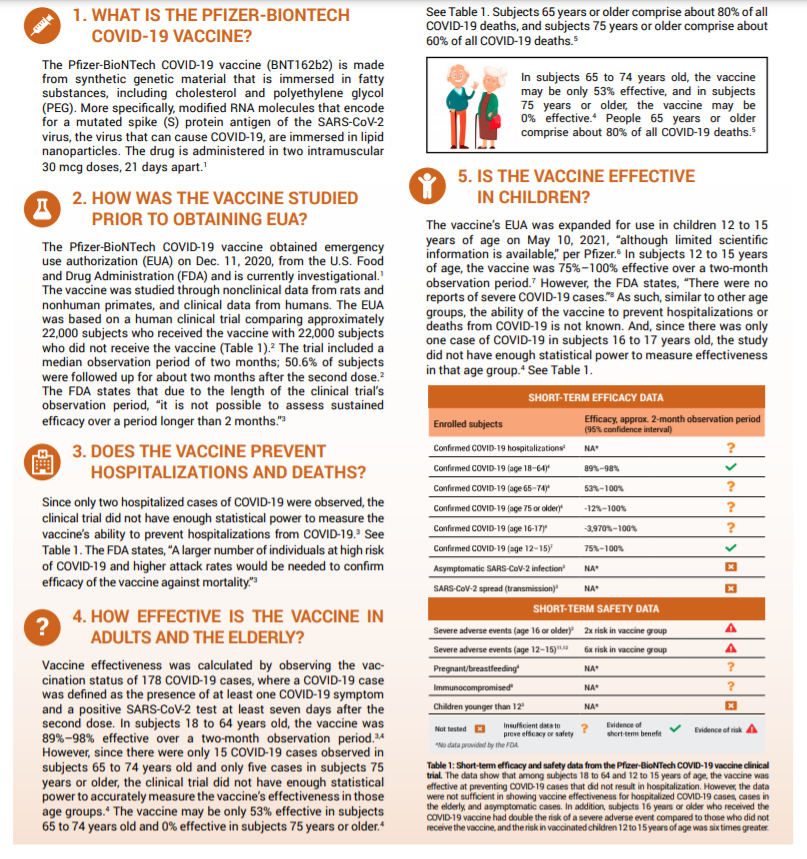
6) “The vaccination doesn’t reduce transmission”
Transmission reduction data against the delta variant is now available. Studies show efficacy against transmission ranges from 50 – 78% – against delta.
But you know what is very effective in reducing transmission of viral illnesses? Masks. See my blog post/mini review on them I posted earlier.
https://www.bmj.com/content/374/bmj.n1960
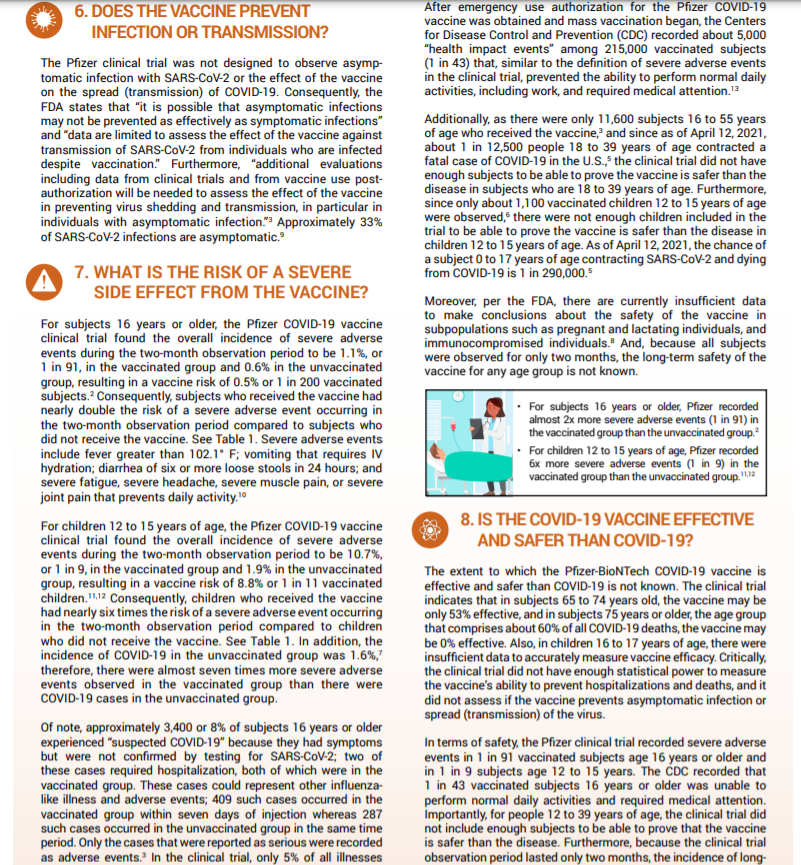
7) “Serious adverse effects are high.”
Serious adverse effects – they included things like muscle and joint pain, which occurs in 25% of patients and 17% of patients. Pain does suck, but it’s highly subjective. Other events included and mentioned first like diarrhoea and vomiting. Diarrhoea occurs in 1/10 COVID patients by ways of comparison. 0.07% of patients vomited after vaccination, 0.12% got diarrhoea (1/1000 or so). The source they referenced for this was a Pfizer vaccine trial’s clinical protocol which has no results, so I’m not sure where these numbers even came from.
We know incidence of things like myocarditis due to the vaccine are 1/100,000, and 0 deaths occured from this over 2million vaccines.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2773790
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7141637/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8152224/
https://jamanetwork.com/journals/jama/fullarticle/2782900
8) “COVID-19 is less dangerous than the vaccine.”
Finally, they end this suggesting vaccines are more dangerous than COVID in young patients, rehashing data they’ve made from invalid assertions earlier, that have been proven since in numerous studies done on young people, and old people. Long term safety data on vaccinations weren’t available then, but they are now. Long COVID studies are coming out though – and the consequences are dire. Studies show that 60 days after infection, 87% of people still had a COVID 19 symptom, with 55% having 3 or more. Scarring is present in the lungs of many. 20% of people hospitalised – which with delta, we’re seeing is occurring in younger patients – have permanent pulmonary fibrosis. Over 70% who are ventilated show this after 4 months.
https://thorax.bmj.com/content/early/2021/05/13/thoraxjnl-2021-217031
Ultimately, we know this disease kills the unvaccinated more than any other groups – 99.5% of people who have died are unvaccinated. It’s not only killing people directly, but also people like me who are at risk, and need things like oral cancer biopsies (which I can’t get here in Aus as elective procedures are shut down).
https://www.forbes.com/sites/jemimamcevoy/2021/07/01/995-of-people-killed-by-covid-in-last-6-months-were-unvaccinated-data-suggests/?sh=6daccc9f493d
References:
- https://www.nature.com/articles/s41586-021-03738-2
- https://onlinelibrary.wiley.com/doi/10.1002/cti2.1319
But I have a LOT of questions that I guess only patients can answer. The little, tiny things – like:
1) Where and how do you prick (for insulin and blood glucose monitoring) EXACTLY to minimise pain?
2) Got any ideas of what things I can eat? I’m low carbs AND low fat.
3) I went really low, blood sugar wise, after exercising a chunk the other day. Even when I’m on insulin, how do I manage this? Should I keep some #gatorade or #jellysnakes at all time and take them when I’m feeling tired?
4) I’ve got a severe autoimmune-like disease, how do I tell if I’m hypo, or just having a bad day, or flare up?
5) Any devices or recommendations you can make for this all?
6) Is there an app for all this (the blood sugar app is OK, but like what works for you guys)?
7) Any good resources? Anyone I should follow with this?
8) What are your anecdotal experiences of medicines etc? (Don’t give medical advice in the comments, but do share your personal experiences!)
I just have a LOT of questions. NikhilAutar.com/diabetesnow, I’ll try and compile the answers.
But I’ll try and share as I learn as well, because though I thought I got it, there’s so many tiny things that are confusing with this disease. But I’m getting there. One thing I’ve been doing – I’m cooking a lot now. And it’s been fun, being able to cook without cutting myself and feeling tireder after a meal (since my cramps are a LOT better). I’ll share those recipes too, because they’re actually so good!
#Diabetes #T2dm #Diabetic #newlydiagnosed #spoony #chronicillness #newdisease #spoonie #cancerlyf #lol #medicine #doctor #medschool See Less

Biden’s Allegations of corruption;
https://fortune.com/2020/10/23/trump-biden-debate-2020-election-corruption-china-ukraine/
Trump approves pipeline he had at least $1-2million investments in.
https://www.theguardian.com/us-news/2016/dec/02/donald-trump-dakota-access-pipeline-support-investment
The leader of the free world sells beans.
https://www.thecut.com/2020/07/trump-goya-beans-photo-fiber.html
Trump golf count; it only calculates the cost of travel, by the way. The actual charges Donald charges his own hotels for his trips (which is quite high) is equally astronomical.
https://trumpgolfcount.com/QD
Ivanka Trump’s brand that was promoted by the press secretary.
Trump leases his own officer for $2.4million from 2017 – 18
https://www.newsweek.com/government-paying-trump-tower-presidential-protection-638852
Jared Kushner and Trump’s business advisor taking almost $1billion directly from their first trip to Saudi Arabia.
https://www.bloomberg.com/news/articles/2017-05-26/the-kushners-the-saudis-and-blackstone-behind-the-recent-deals
https://www.vox.com/policy-and-politics/2019/9/17/20868358/donald-trump-saudi-money
Further Trump ties to Saudi Arabia which started decades ago.
https://www.businessinsider.com.au/trump-saudi-arabia-financial-interests-ties-hotel-bookings-sales-2018-10?r=US&IR=T
Kushner’s sister sold Visas to Chinese businessmen for $500,000 investment into their business.
https://www.washingtonpost.com/world/in-a-beijing-ballroom-kushner-family-flogs-500000-investor-visa-to-wealthy-chinese/2017/05/06/cf711e53-eb49-4f9a-8dea-3cd836fcf287_story.html
This reportedly increased to $3million/year around America after the first 18 months. He also claims COVID-19 relief for this.
The Saudi $1.4billion bailout of the Kushner family, right as a $1.4bn mortgage payment was due.
https://www.vanityfair.com/news/2019/02/qatar-666-5th-ave-jared-kushner
This directly led to Trump changing his stance from calling them a terrorist state to saving them from a war that would have destroyed them.
https://www.aa.com.tr/en/americas/qatar-trump-retreats-from-supporting-blockading-states/1988095
Tom Price buys $90,000 in pharma stock just before passing policies which further increased patent protection for them.
https://psmag.com/news/tom-prices-investment-portfolio-benefits-from-his-pharma-agenda
Michael Flynn takes $33,000 from Russia Today – one of the largest promoters of fake news in 2016.
https://www.usatoday.com/story/news/2017/03/16/michael-flynn-received-more-than-33000-russian-tv/99258514/
Steve Bannon steals $1.4million from a Go Fund Me for the border wall (through channeling it into his not for profit, and spending on himself.
https://www.abc.net.au/news/2020-08-21/former-trump-adviser-steve-bannon-arrested-fraud-conspiracy/12580952
]]>
A Ted Talk I’ll be watching tonight! The paper on this, I have read, and is linked below.
A report on the benefits of patient centered care – a model that advocates you involve patients in their care decisions, and that you provide both physical and emotional comfort to patients.

As it is Christmas today, I thought I’d share the best gift I’d ever gotten.

Bachelor of Medical Research (WSU).,
Bachelor of Medicine, Bachelor of Surgery (WSU 2023).
Permanent Lung Damage is Almost Certain To Occur in Many COVID19 Patients.
Even mild infection can incapacitate healthy people for MONTHS.
It’s almost certain that COVID19 causes permanent lung damage in a large proportion of seriously ill patients. Young, fit and healthy people, including athletes, are not spared, and indeed, likely to suffer most (at the very least, they suffer for the longest). There’s a bit of evidence that those putting their body through extreme strain are more inclined to suffer worse outcomes when it comes to pneumonias. I felt my favourite stars, in my favourite sport, that I can no longer play due to severely damaged lungs, should know this information. Though important causes like the recent Black Lives Matter marches are indeed of concern, to both protect themselves, and the millions of young and old fans they have, it would be amazing if players could help spread this message – to distance, where possible, and do things like wear masks. Trust me – permanent lung damage sucks. I’m 26 and likely will never play basketball again.
This medical journal of Australia review of radiological findings of COVID19, suggests up to 17% of severely ill or critical patients1 , not just those requiring ventilation, have evidence of fibrosis – permanent lung scarring in the lungs. A more recent analysis of 38 patients’ autopsies showed all patients who did require critical care had signs of this2. Though younger people do survive COVID-19 more, the question is at what cost?
A 15 year follow up of SARS coronavirus patients also confirmed that as many as 4.6% of a mostly healthy population had decreased lung function after any level of SARS infection2. Some are suggesting that this likely isn’t progressive fibrosis, which is good news in that it is not likely to cause long term inflammation in the lungs3, but a recent study in the Lancet suggests otherwise – and indeed, cites higher rates of developing fibrosis than earlier thought4. Also, permanent disability and lung function is demonstrated through previous coronavirus outbreaks’ data, and through studies on radiological findings of the current pandemic – which suggests as many as 17% of severely ill patients are demonstrating signs of fibrosis1 (this number are likely to rise on follow up.
Elite athletes are at higher risk of contracting COVID-19. Not only can exercise direct this particularly pneumo-toxic virus deeper into lungs, which may lead to higher chances of developing cytokine storms, and a more severe version of COVID-195, extreme exertion may reduce innate immunity, making players more prone to developing disease6. Not only is there this chance of permanent lung damage which could affect entire careers, It also appears that even mild infection commonly leads to a 20-30% decline in lung function that lasts for months12 – longer than the common flu – which could impact these very finals.
PLEASE – keep yourselves safe! Not just for your own sake, but also for others.
Children, though less likely to suffer from severe illness, are being admitted to ICUs in 0.58-2% of cases, according to CDC numbers in the US6, and the most comprehensive study on paediatric outcomes out of China7. It’s also evident that infants under 1 are at significantly higher risk of ICU admission (4x that of other children)7, and thus, exposure to this permanent damage. Not only is this linked to permanent lung damage, ICU admission causes severe trauma and PTSD too.
Many children follow sports stars religiously. Hopefully getting messages out to them and their families will keep, and the world at large, will keep them more safe.
It is concerning to see that sending children back to school is being encouraged by governments such as Australia8, against medical consensus. Opening up is occurring in the US too. Young people are similarly being asked to sacrifice themselves to attain ‘herd immunity’ around the world, athletes are being sent back into action. Though many are wary, as evidenced by Novak Djokovic’s diagnosis and disregard for social distancing, many aren’t spreading the right message, and may well be putting their teammates’ careers at risk.
Not are there much higher rates of ICU admission and deaths being seen in 20-44 year old age groups (up to 12% for the former)10, long term deleterious side effects of this through things like lung fibrosis is likely, and could have even worse economic outcomes in the long run too.
It’s not to say we shouldn’t reopen. But we should definitely be encouraging safe habits like mask usage and social distancing – staying in unless necessary, or if public health bodies say it’s okay to – to minimize the damage. Not only to athletes’ careers, but to the world as a whole. This disease could be worse than we imagine. I just hope we can encourage eachother to stay safe.
I am an ex cancer patient, and extensive treatment has caused significant, permanent lung damage to me. My lung function is similar to levels seen in early studies of patients who were followed up after SARS-CoV-2 infection (a 20-30% reduction). I likely will never get to play basketball, or run, again. And though data as to extent of pulmonary fibrosis isn’t available yet, this data makes it clear that fibrosis is occurring. This is not something we want to expose multiple young generations to.
References;
- Peter G Gibson, Ling Qin and Ser Puah, COVID-19 ARDS: clinical features and differences to “usual” pre-COVID ARDS, Med J Aust, Published online: 24 April 2020, accessed May 2020, available at https://www.mja.com.au/journal/2020/covid-19-ards-clinical-features-and-differences-usual-pre-covid-ards
- Zhang, P., Li, J., Liu, H. et al.Long-term bone and lung consequences associated with hospital-acquired severe acute respiratory syndrome: a 15-year follow-up from a prospective cohort study. Bone Res 8, 8 (2020). https://doi.org/10.1038/s41413-020-0084-5
- Pulmonary Fibrosis Statement on COVID-19, Pulmonary Foundation Press Release, accessed May 2020, Available at https://www.prnewswire.com/news-releases/pulmonary-fibrosis-foundation-statement-on-covid-19-301035924.html
- P Spangnolo, E Balestro, S Aliberti, E Cocconcelli, D Biondini, GD Casa, N Sverzellati, TM Maher, Pulmonary fibrosis secondary to COVID-19: a call to arms?, Lancet Respir Med. 2020 May 15, doi: 10.1016/S2213-2600(20)30222-8 [Epub ahead of print]
- P Matricardi, RD Negro, R NIsini., The First, Comprehensive Immunological Model of COVID-19: Implications for Prevention, Diagnosis, and Public Health Measures, Version 1 : Received: 22 April 2020 / Approved: 24 April 2020 / Online: 24 April 2020 (10:25:27 CEST)
- S Estruel-Amades, M Camps-Bossacoma, M Massot-Cladera, FJ Perez-Cano, M Castell., Alterations in the innate immune system due to exhausting exercise in intensively trained rats, Sci Rep 10, 967 (2020). https://doi.org/10.1038/s41598-020-57783-4
- Bialek S, Gierke R, Hughes M, McNamara LA, Pilishvili T, Skoff T., Coronavirus Disease 2019 in Children — United States, February 12–April 2, 2020, MMWR Morb Mortal Wkly Rep. 2020 Apr 10; 69(14): 422–426.
- Dong Y, Hu Y, Qi X, J Fang, J Zhongyi, Tong S., Epidemiological Characteristics of 2143 Paediatric Patients With 2019 Coronavirus Disease in China, Paeiatrics, Pediatrics April 2020, e20200702; DOI: https://doi.org/10.1542/peds.2020-0702
- Birmingham K., South Australian parents encouraged by Education Department to return children to school amid coronavirus pandemic., ABC News, April 22, Accessed May 2020., Available at https://www.abc.net.au/news/2020-04-22/sa-parents-urged-to-send-children-to-school/12174872
- Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) — United States, February 12–March 16, 2020. MMWR Morb Mortal Wkly Rep 2020;69:343-346. DOI: http://dx.doi.org/10.15585/mmwr.mm6912e2
- Doherty B, Taylor J, Remeikis A., NRL Announces 20-Round Competition Restarting on 28 May – as it Happened, The Guardian, 28 April, Accessed May 2020., Available at: https://www.theguardian.com/australia-news/live/2020/apr/28/coronavirus-australia-update-latest-bondi-beach-reopens-to-swimmers-as-new-cases-drop-to-single-figures-live-news?page=with:block-5ea7da968f086f39b4ca135d
- Cheung E., Coronavirus: some recovered patients may have reduced lung function and are left gasping for air while walking briskly, Hong Kong doctors find., South China Morning Post. Accessed May 2020, Available at https://www.scmp.com/news/hong-kong/health-environment/article/3074988/coronavirus-some-recovered-patients-may-have