The full document they put out can be accessed here. Or just scroll down. I’ll break these down point by point –
2) “The vaccine was approved early. It did not show long term efficacy.”
Yes, it was approved early, but this was due to it being an emergency. Significant data on safety had been gained prior to this, and efficacy was demonstrated to be very high through a trial with rigorous design, and COVID had killed hundreds of thousands in America alone to this point. There’s a reason this provision in FDA regulations exist. We are still collecting data on long term efficacy, but it’s been demonstrated regularly that long term immunity is formed after COVID-19 vaccination[1, 2].
https://onlinelibrary.wiley.com/doi/10.1002/cti2.1319
https://www.nature.com/articles/s41586-021-03738-2
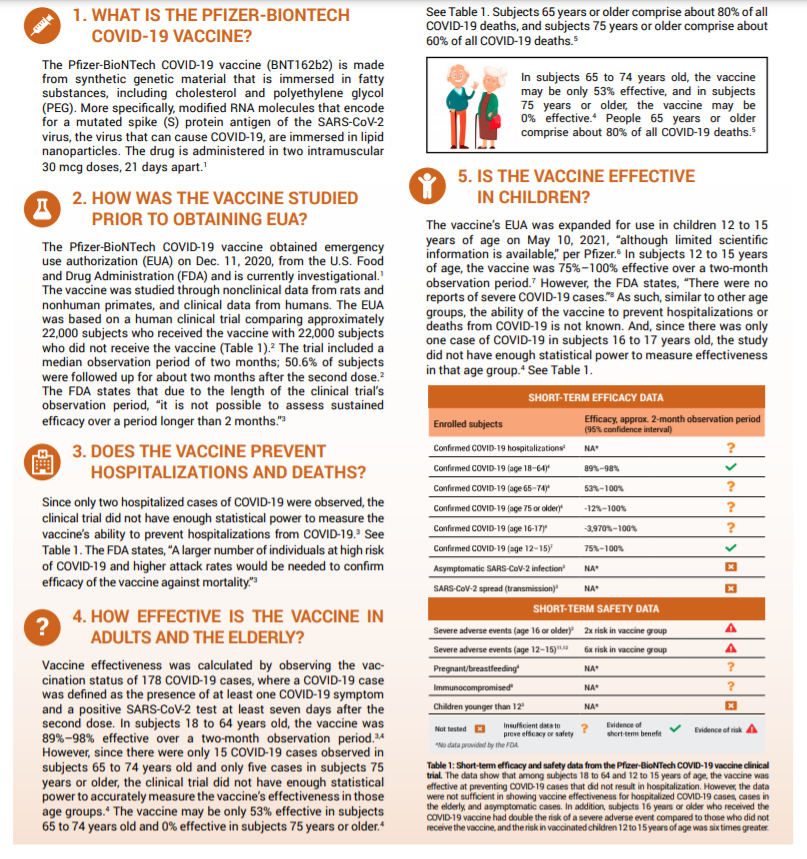
3) “You didn’t get enough of a sample size and some age groups weren’t sampled.
So this is the thing. Vaccine studies don’t even need that many participants to get statistical power to make an apt conclusion. This study had MORE than enough (you need 10-15k to get statistically significant results typically). COVID-19 vaccine studies that led to Pfizer getting emergency approval had over 20,000. To this day, 4.5 BILLION DOSES HAVE BEEN ADMINISTERED to 31% of people in the world! This is no longer an experiment.
The fact that only 2 patients in younger groups got COVID doesn’t mean it’s statistically insignificant, it means the vaccine is very effective. You compare the numbers in both cohorts, and see how much of a reduction there is to calculate vaccine efficacy. So that part too, is wrong. In later ones they make further claims about lack of vaccine efficacy,
This study on the 2018 influenza vaccine enrolled 10,000 people. This one did 3600. That’s more than enough. If anything this had even more proof than most. It was approved for emergency use due to there not being long term data on efficacy. Safety wise, vaccines are very largely very very safe.
https://cdn.pfizer.com/pfizercom/2020-11/C4591001_Clinical_Protocol_Nov2020.pdf
https://ourworldindata.org/covid-vaccinations?country=OWID_WRL
https://clinicaltrials.gov/ct2/show/NCT00711295
https://pubmed.ncbi.nlm.nih.gov/33065035/
4) “This is NOT shown to be effective in older adults.”
You could make that argument as mainly younger patients were included in this study, but since the approval, we’ve gained a lot of data on this. 156000 patients over 70 were studied in this BMJ trial that showed 95% efficacy. This review found similarly high results.
https://www.bmj.com/content/373/bmj.n1088
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8024166/
5) Not effective in teens.
Subsequent studies on this exact age group cited as a concern by this group of ‘physicians,’ (12 – 15 year olds) show very high efficacy of 100%.
This is not being seen now as we see many younger patients being infected with the delta variant. 30-40 year olds have 4x higher risks of death compared to 18 year olds. This is affecting more young people, likely because vaccination rates are not as high in these populations. And the delta strain seems to be more dangerous. So vaccinate!
https://www.bmj.com/content/373/bmj.n881
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html
6) “The vaccination doesn’t reduce transmission”
Transmission reduction data against the delta variant is now available. Studies show efficacy against transmission ranges from 50 – 78% – against delta.
But you know what is very effective in reducing transmission of viral illnesses? Masks. See my blog post/mini review on them I posted earlier.
https://www.bmj.com/content/374/bmj.n1960
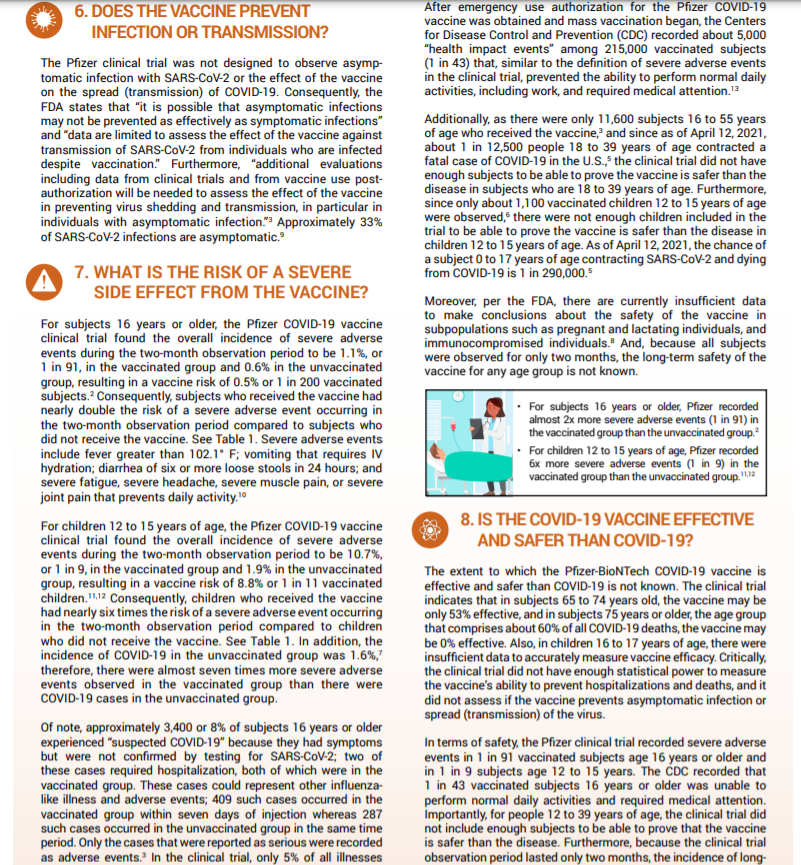
7) “Serious adverse effects are high.”
Serious adverse effects – they included things like muscle and joint pain, which occurs in 25% of patients and 17% of patients. Pain does suck, but it’s highly subjective. Other events included and mentioned first like diarrhoea and vomiting. Diarrhoea occurs in 1/10 COVID patients by ways of comparison. 0.07% of patients vomited after vaccination, 0.12% got diarrhoea (1/1000 or so). The source they referenced for this was a Pfizer vaccine trial’s clinical protocol which has no results, so I’m not sure where these numbers even came from.
We know incidence of things like myocarditis due to the vaccine are 1/100,000, and 0 deaths occured from this over 2million vaccines.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2773790
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7141637/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8152224/
https://jamanetwork.com/journals/jama/fullarticle/2782900
8) “COVID-19 is less dangerous than the vaccine.”
Finally, they end this suggesting vaccines are more dangerous than COVID in young patients, rehashing data they’ve made from invalid assertions earlier, that have been proven since in numerous studies done on young people, and old people. Long term safety data on vaccinations weren’t available then, but they are now. Long COVID studies are coming out though – and the consequences are dire. Studies show that 60 days after infection, 87% of people still had a COVID 19 symptom, with 55% having 3 or more. Scarring is present in the lungs of many. 20% of people hospitalised – which with delta, we’re seeing is occurring in younger patients – have permanent pulmonary fibrosis. Over 70% who are ventilated show this after 4 months.
https://thorax.bmj.com/content/early/2021/05/13/thoraxjnl-2021-217031
Ultimately, we know this disease kills the unvaccinated more than any other groups – 99.5% of people who have died are unvaccinated. It’s not only killing people directly, but also people like me who are at risk, and need things like oral cancer biopsies (which I can’t get here in Aus as elective procedures are shut down).
https://www.forbes.com/sites/jemimamcevoy/2021/07/01/995-of-people-killed-by-covid-in-last-6-months-were-unvaccinated-data-suggests/?sh=6daccc9f493d
References:
- https://www.nature.com/articles/s41586-021-03738-2
- https://onlinelibrary.wiley.com/doi/10.1002/cti2.1319
And sign up to my email list (I don’t post often, but you’ll be notified when I do this way!).
Bone Marrow Transplants
The bone marrow transplant procedure, in a nutshell, is basically getting someone else’s blood stem cells (haematopoiec stem cells is the technical name), located in their marrow, and infusing it into you, so it settles. They aim to get someone else’s immune cells in you, to kill off your cancer (your immune cells are made by your blood stem cells). And the major side effect, other than the dangerous infections you can get during the procedure and in the first 30 days due to, largely, chemo, is graft versus host disease, which can last a long time in others (but in small doses, is actually a good sign the process is working).
How it works for the donor – it’s taken peripherally from the arm, after getting a medicine which makes those stem cells enter your circulating blood for a few weeks (click here to learn about that).
On the recipient’s end, you receive it through an infusion into your veins, in most all cases. It eventually finds it way into your marrow and starts producing your donor’s blood cells (including white, immune cells), after a few weeks (it took 3 weeks for mine to engraft on both occasions, but it can vary).
The idea is, though you and your donor are matched as well as you can be – there will always be slight differences between you and them, which makes them recognise cancerous cells and kill them off, where your immune system may have lost the ability to do. This is a good thing in that it’s how the BMT or SCT (stem cell transplant) is supposed to work. But it also is the cause of the major side effect, graft versus host disease, where your donor’s cells attack your own organs. I’ll get to that later, here’s how it all goes though.
Prior to the transplant, you receive workup of some kind – often they want to ensure your underlying disease is under control. If it’s a blood cancer, often that will involve chemotherapy. Once they have the disease and any underlying conditions mostly under control, and they find a match, and coordinate timings (usually, you want to get the donor’s cells into you as soon as it’s taken from them), they begin the workup to the actual stem cell transplant process.
Usually, a week or so before, they’ll begin immunosuppressive regimens and chemotherapy that are designed to kill off your current immune cells. In younger patients, they may also offer total body irradiation, which is a high dose of radiation given to your entire body (in younger people, marrow can be produced all over the body, so all areas are targeted, though they will provide shielding to your brain and lungs, in most cases). The idea is to kill off your old bone marrow’s cells and replace them with your donors’.

I won’t lie, the BMT process and chemotherapy is tough. But it is lifesaving. Definitely listen to your doctors!
During the next few weeks, like many chemos, you will have a lot of your immune cells and your blood cells obliterated. So you’ll be very susceptible to infections. It is very important to do everything you can to avoid infections in this time, from limiting visitors (especially sick ones), to cleaning and bathing regularly (even when you won’t feel like it) and following your doctors’/nurses’ orders. You also may experience other side effects such as nausea, gut pain (from your stomach lining cells dying off), fatigue and general unwellness. There are many chemotherapy specific side effects too that may occur, and you may also get other side effects – eg. with TBI (total body irradiation), you often get mucositis – inflammation of your mouth and throat – which can be extremely painful. I’ve personally experienced this myself and highly recommend you follow doctors’ suggestions and get ENG tubes if they think it’s appropriate and helpful, and getting pain teams to come in and help too. Having said that – my second transplant was a ‘reduced intensity chemotherapy’ regimen. I only had nausea and didn’t get an infection once, and it went quite smoothly compared to the first. Everyone’s different, every regime is different, and even in one person, at different time points, you can react differently.
Other things they may do in your workup/the month before your transplant, is check your heart, and lungs, and, if you’re in that age category, your fertility. They’ll put a line in just before they begin treatment in hospital, this may be in your arms, or via ports they put into your neck. During the transplant, and the immediate transplant workup, they’ll watch over you, do bloods regularly, get scans when required, and treat things like infections. Infections are often the most dangerous thing you may face, but they’ll be sure to give you antibiotics, and other treatments, as required during this time frame.

This is the TBI – total body irradiation process. This is usually done in younger patients, as they are more likely to have marrow that persists in other bones of your body (adults often only have it in their sternum and hip bones). Hence why they shoot radiation at your entire body (left of this photo is a machine which does this). The rice bags keep you still and provide some protection to important organs like your brain and lungs. And they keep you still. It lasted 30 minutes, and I had 5 sessions over a week at a special clinic the week before my transplant). Straight after you may get a burning sensation in the skin (this is resolved by creame in most cases). The other common side effect is mucositis, a sore throat, which can be very painful. So listen to your doctors if they recommend a feeding tube! I learned that the hard way!
At some point, often 3 – 4 weeks after “Day 0,” where they infuse you with your donor’s cells, you’ll ‘engraft’ and have your donors’ cells start making cells in your blood. They’ll be monitoring for this. After this, a good number of people get acute graft versus host disease, which can affect any of your organs, and can be pretty severe. This occurs in the first 90 days usually, and can affect any of your organs – from your skin, to eyes, to liver, to gut. I personally had bad skin and liver and gut GVHD (in my first transplant, I had skin and liver aGVHD, and in the second, liver and gut aGVHD). Not everyone gets GVHD. It can be a good sign that you’re getting the ‘graft versus disease’ effect too (where your donor’s cells kill off/stop your cancer cells from returning), but too much GVHD can be bad too. Your doctors will treat you after you engraft with some medicines that suppress your immune system – often cyclosporine, but different doctors/patients use different treatments. If GVHD manifests and gets severe, they may add more or increase your dose. Or they may reduce them over time.
You’re still not out of the woods after this time frame. You can get infections, still. And with GVHD – days can be critical when it comes to your outcomes, so make sure you tell them of anything you may experience. With different organs, you may experience different signs. Eg – with the skin, you may get rashes or feel like your skin is burning. With the gut, you may get diarrhoea, sometimes constipation. With the eyes, you may get burning or find it difficult to open your eyes (which may be due to skin GVHD affecting the skin around your eyes). It varies from person to person. It’s VERY important you see your doctors if something happens. But sometimes, you won’t feel anything. With my liver graft versus host, I didn’t feel a thing, but had very very high liver enzyme tests.
I couldn’t find a clean, clear photo of my skin, so sorry for the captions. But this is chronic skin GVHD – I have quite severe chronic GVHD and it’s not too bad, other than the looks (I don’t mind the looks though – this is how I dealt with the social anxiety that comes to many post transplant, due to the change in looks). Acute skin GVHD can be more red and flared, and may occur anywhere. It may burn or itch. I know it’s hard, but try not to itch! But right now, as someone with chronic graft versus host disease, I can’t feel it, it isn’t painful, but it may make my skin less elastic, and does impede my joints a little bit. But I’m largely OK now!

Usually, they’ll tell you to come into hospital as soon as possible if you get a fever or infection symptoms of any kind. With COVID-19 going on right now, clarify with your doctors if or when to come in. Many hospitals, including mine, will give you a card to get you into ED faster. Even after the pandemic ends (which may not be for years officially), it may be wise to wear a mask and avoid crowded areas too.
Depending on your donor and your status, you may also get exposed to viruses that may put your graft (your transplanted cells) at risk. Your doctor will likely have you on prophylactic, preventative, antivirals, antibacterials, and maybe antivirals too to prevent this. And they’ll likely check your levels of various medicines, and monitor for these viruses too. This is why it’s really important to see your doctors and get your blood tests as much as they want you to. Hopefully, this will go from weekly appointments to fortnightly, to monthly, to 3 monthly, to yearly. And then comes long term monitoring.
You also generally feel tired. I did after both transplants for months. Some of the medications you may be put on have annoying or frustrating side effects – eg. prednisone is a steroid medication (not the muscle building type unfortunately), which can make you angry, make it hard to sleep, and make you gain weight. But it’s also lifesaving. It’s important to keep in touch with your doctors to monitor this.
![]()
The way cancer changed me used to really impact my mental health. To the point where, even though it was harmful for my health, I didn’t want to go out because of how it affected my looks. This is me years afterwards, but straight after chemo, on 100mg of prednisone, I had the classic “chipmunk face.” But I got over that after a while. This is how. I hope it helps those of you who may suffer from this out too.
After 3 months, you may also develop chronic graft versus host disease (cGVHD), which may manifest all over your body, and may get severe too. it’s important, once you get signs of anything weird, to tell your doctors about this so they can treat it, again. And treatment may last longer or be chronic, as the name implies. I still have some, 8 years out. But again, everyone’s different in this. I’ll make a post about this later – but there are many organs it can impact, from your skin, to eyes, to lungs and in rare cases, even heart. It’s important to get on top of this early. But the good news is, in many patients, it either ‘fizzles out’ or ‘plateuas.’ But without treatment, it can worsen, even after you’ve got it under control. So stay connected to your doctors and listen to their advice!
That’s the transplant process, in summary. I know it’s a lot of information. But the main thing, is it a marathon. But it is also curative – it was one of the first curative options we had for any cancer. Though it can be dangerous, it has a good chance of fixing many diseases. Your doctors wouldn’t be doing this to you if they didn’t think it could help.
I hope it makes sense. Let me know if you have any more questions. And sign up, do email me at info at nikhilautar dot (com) with any questions, and stay in touch!
But they don’t make you bulletproof.
I’m writing this because I’ve seen and been talking to a couple of very high risk friends, one who’s actively getting cancer treatment, the other halfway around the world, going out with masks. When I asked one – a friend who is on chemo (I was shocked that he was going to a stranger’s birthday party while Melbourne’s lockdown was going strong) – he said that did so because he’s wearing a mask, and that he should be fine. He’s either using a mask as a justification, or going out because of the mask.
It’s nuanced. It’s not easy to communicate, because we do want people wearing masks when they go out. But for years, its been suggested that we shouldn’t be giving people a false sense of security with mask usage[1,2]. The WHO didn’t make this suggestion out of the blue, as many on #MedTwitter suggest. Even studies modelling mask usage controlling the virus mention this[3].

There is evidence showing that this isn’t just conjecture too. This study used a location app to track individuals’ habits in mask mandated areas vs non mask mandated one. Those in mask mandate regions spent 20-30 less minutes at home, and more time in commercial locations directly after the mandates! It could be contributing to spread if there aren’t further measures taken by cities [4]. To be fair, this is a preprint, but unless it’s fraudulent, or sample sizes are incredibly small, a sharp drop in household days after mask mandates were given is telling. Perhaps it’s the mask mandates as opposed to the mask which got people to want to go out more. But that points to communication being an issue!
On the other hand, there is a review which suggests that mask doesn’t increase the risk of people going out that went viral. But though the medical world latched onto this, the study only showed that mask usage didn’t reduce handwashing. It didn’t (because frankly, it hasn’t been studied until recently), find if mask usage increased distancing[5].
I’m not saying that you shouldn’t wear a mask! The very opposite. Mask usage likely does reduce your risk of contracting a virus, and it IS definitively, through many studies, shown to reduce transmission if you happen to be ill in the community [7-9]!
But we should be telling people to wear a mask – IF You need to go out.
ESPECIALLY to those at higher risk. As many as 50% of the population in developed nations have a risk factor that increases mortality risk with COVID-19. There are many dying in their 30s. Long term complications are still not known!
If you’re at risk – Please, where possible, avoid going out if coronavirus is raging in your area. Listen to local health bodies and your doctors. That mask WILL reduce your risk most likely when you NEED to leave the home. And it can’t hurt you. But you shouldn’t be convinced that it will protect you. Even if you’re protesting a very good cause – if you or loved ones you interact with are at risk – I’d suggest you stay home.

The fact is – the WHO came out early on not recommending masks, as did many other nations, because the small studies that have been done on them show that in community settings – mask usage doesn’t reduce your risk of infection.
This RCT showed that it didn’t reduce your risk of catching disease significantly in younger populations[6] This RCT showed difference either – though its primary aim was to look at household transmission reduction, it showed that influenza like illness (a primary way flus are tracked) contraction was similar in mask/non masked groups [10]. They definitely DO reduce your risk of contracting illness, if they’re fitted n95s where users are trained in their use, as this review shows[7]. But that’s very different from community use.
Though countries like China and Japan are pointed to as proof of masks working, a study of Japanese mask usage has actually shown that it’s not masks, but rather the differing habits of mask/non mask users, that lowers their risk of contracting viral illnesses. People who wear masks tend to go out less, and wash their hands more than non mask wearing counterparts[11]. A similar study of Hong Kong residents found similar results[12].
But again, they definitely reduce your risk of transmitting disease to someone else, as I mentioned above[7-9]. And though statistically significant lowered rate of infection in these community studies wasn’t reached – you need up to 10,000+ people to get surveys like this to have statistical power (though this was an RCT, 1000 people to track a whole populations’ risk of flu may not be enough) – reductions in mask groups were seen.
Various lab bench/cough-simulating studies, like this one where outward particle emission was reduced by 90% on speaking[13], and common sense, we can tell that it will likely reduce your risk of contracting illness from droplets at the very least – even if it only stops you from touching your face as much[14]. But there are some studies disputing that masks even lower transmission with SARS-COV-2[15].
That’s why I emphasise, if you’re at higher risk – your best course of action is to stay away from sick people in the first place!
If you want to subscribe to an email list that’ll let you know if you can help scientists answer easy questions – check out CAroundYou.com/ProveIt
References;
I’m not gonna bother referencing properly as I’m not on my desktop which has EndNote, but should – I may later.
1) https://www.bmj.com/content/369/bmj.m2003
2) Culture matters a lot when it comes to mask usage and its efficacy. Really interesting look into this;
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4868614/
3) https://royalsocietypublishing.org/doi/10.1098/rspa.2020.0376
4) https://www.medrxiv.org/content/10.1101/2020.05.23.20111302v2
5) https://www.bmj.com/content/370/bmj.m2913
6) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3266257/
7) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5779801/
8) https://pubmed.ncbi.nlm.nih.gov/19193267/
9) https://pubmed.ncbi.nlm.nih.gov/18461182/
10) https://www.acpjournals.org/doi/full/10.7326/0003-4819-151-7-200910060-00142
11) https://pubmed.ncbi.nlm.nih.gov/23227885/
12) https://pubmed.ncbi.nlm.nih.gov/16318726/ – like Japanese study.
13] https://www.nature.com/articles/s41598-020-72798-7
14) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7321045/
15) https://www.acpjournals.org/doi/10.7326/M20-1342
]]>

Pictured here, your average Karen, freaked out by the Corona-virus. Should she, though?
How Lethal Is It? – More lethal than the flu, but numbers will likely change over time.
The latest information we’ve gotten directly from, largely, the Wuhan Epicentre (the numbers come from the Chinese Centre of Disease Control and Prevention) of disease shows that out of 72314 cases studied, there was an overall mortality rate of 2.3%. No deaths have been recorded in those aged 0-9, but deaths do increase exponentially with age, which is to be expected with many viruses of this type (peaking at a 14.8% mortality rate in those over 80). It’s important to note that an association with healthcare burden and death has been demonstrated in this virus, with the epicentre and neighbouring towns in the area seeing much higher mortality rates, which basically means, mortality rates could be inflated, as Wuhan exposures did dominate in terms of cases examined here. Poverty as well could skew mortality rates further as well, as is the case with many diseases such as measles. But figures may be downplayed as most cases of disease are mild, and the fact that China’s numbers and reporting of this has been questioned by many.
Though sample sizes are low, as we approach a few thousand people surveyed, it’s likely that overall mortality rates are lower than what’s been seen in Wuhan and Hubei (the province which Wuhan is capital of). The most accurate coronavirus figures are updated regularly and most accurately by John Hopkin’s University.
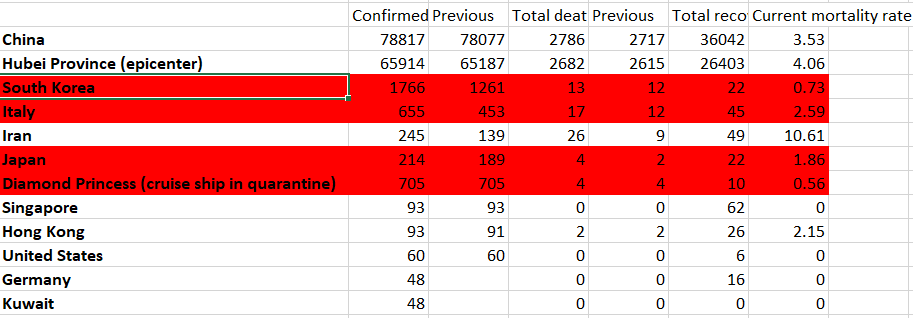
Important to note – Italy and Japan have both been ‘shocked’ by this outbreak and are now responding with vast restrictions, which should reduce incidence and cases. Iran, as you’ll see below, has not been following that example and has a notoriously bad health system to begin with, with some of the lowest number of hospital beds per capita in the world – fitting it directly under the low healthcare resources category described above.
What does Flattening the Curve Mean, and why do we need to control disease early?
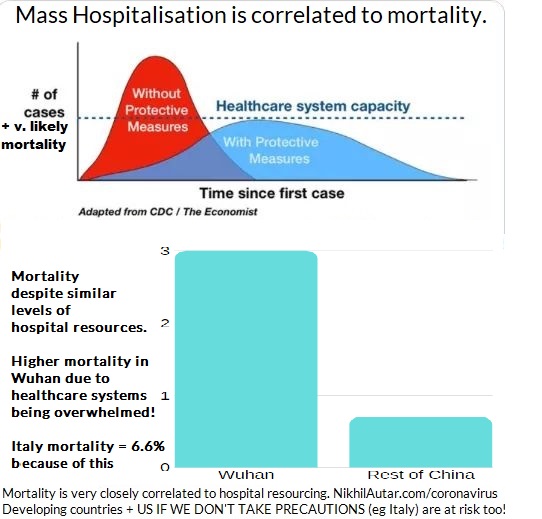
This summarises this best. But basically, the idea of making sure that both cases, and hence mortality, doesn’t exceed hospital system capacity is very important. As demonstrated above, there is a correlation between higher mortality rates and overburdened hospitals. Cases in Italy have been severe, to the point where doctors are being forced to make terribly hard decisions. If we stop the spread, however, we have the chance of not overwhelming hospitals and ICU beds and respirators, which are currently out of stock, and minimizing death.
I heard that China stopped the Spread. Can we do that too?
When the R Number reaches below 1 – disease can no longer spread. China has reached that point – but what remains to be seen if measures that Italy and other nations have taken can stop it in lieu of a vaccine which can help diminish spread or stop it altogether.
Outside of Age, are there any other risk factors? – Yes.
If you have preexisting conditions – the coronavirus could be especially dangerous for you, with mortality rates of 10.5% for cardiovascular disease, 7.3% for diabetes, 6.3% for chronic respiratory disease, 6.0% for hypertension, and 5.6% for cancer. It’s important to note that these diseases are often faced by older people and that these numbers weren’t adjusted for age in the study, but viruses do typically affect the already ill worse, so it’s very reasonable to assume there is a higher risk if you happen to fall under one of these categories.
How fast and far will it spread?
The “R Number” – R0 (the number of people you’ll infect, on average, if you get the disease) has been confirmed to be around 2.3, through a convenient study where 355 verifiably infected people managed to be in a confined space for a few weeks in a row – ideal scenarios for calculating this (which may, if anything, given it was done on members of a cruise ship which is REALLY confined) inflate numbers slightly. which makes it more infectious than the common seasonal flu, and even previous flu pandemics. It’s important to note though that these previous pandemics were in times when diagnoses weren’t high, and that other disease specific factors play into the spread, but though it doesn’t look high compared to other highly infectious diseases presented below – given disease characteristics and the lack of a vaccine, it’s definitely got pandemic potential.
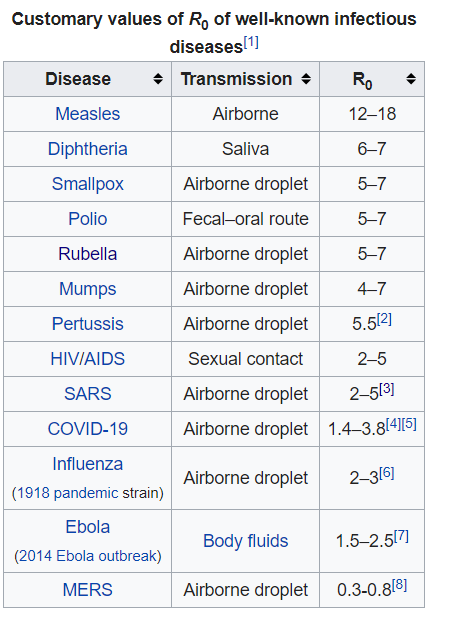
Unlike the diseases ranked higher than COVID-19, COVID-19 does not have a vaccine developed for it yet.
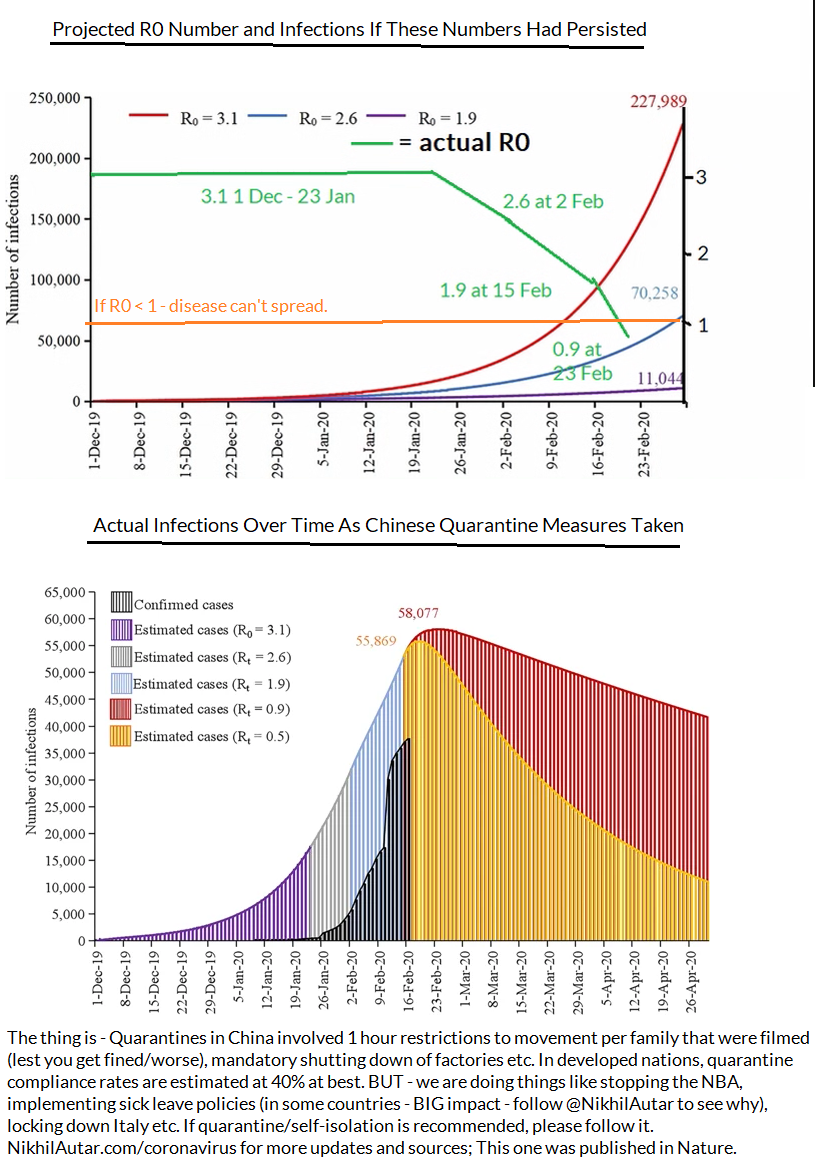
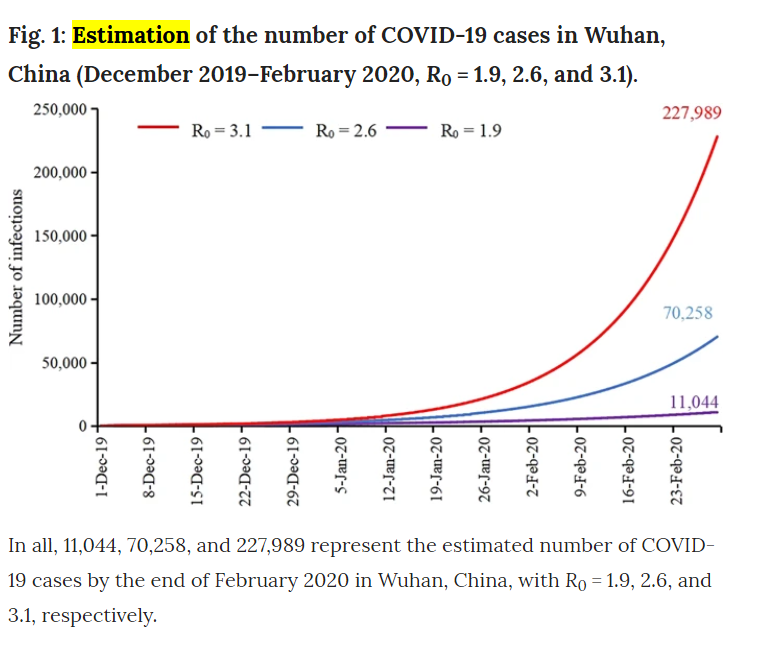
According to estimations made a few weeks ago (between January and Feb 15) on in the course of disease, there should have been less infections as there are now by the middling series of Rt estimates (in this study, they modeled data from January under projected number of cases and estimated that with a R number of 2.6, there should be around 70,000 by Feb 29. As of March 3, there are 80,000 cases in all of China. But with the interventions the Chinese government took, shutting down factories and effectively quarantining a nation, assuming a reduction in R0 as time goes on (which was observed by researchers), we should have peaked by now in terms of novel cases in this district.
Does that mean the spread is stopped? No – there were extreme measures taken in China and Wuhan in particular. But it could mean that R0 has been overblown thus far, likely due to endemic factors such as overburdening of healthcare resources, or poverty. We can’t know for sure right now – in any case, given its propensity to be more lethal
So what do researchers think is going to happen? Well, it’s hard to predict. But given that SARS and MERS, the 2 most recent coronavirus related pandemics we’ve faced, have been less community-spread than this strain of the coronavirus, and that there are numerous cases in the US popping up now where there’s been no contact between the patient and someone around them, there’s a higher chance of this spreading further than those other 2 did, but with lower mortality rates, it could be the case that this won’t be as serious. It’s great to see a coordinated global response behind this. But there are many instances of misinformation going around which is concerning to say the least. For example… it doesn’t help when thousands of pilgrims go around licking statues in Iran, the nation with the second worst outbreak of COVID-19, nor is it safe to go around, kissing people and making contact with random strangers in public, something the Pope insisted on doing despite Italy having the worst outbreak of COVID-19 (at the time of writing this) in the developed world.
Why? Surely Allah has better ways to test faith than challenging you to thumb your nose at what could be a global pandemic… As a nation which sees tens of thousands of pilgrims a day, and one already struggling to cope with the virus (indeed, it hasn’t got amazing healthcare, which, as we demonstrated above, is correlated to worse outcomes), it’s imperative we don’t do stuff like this.
Stopping Transmission And Reducing Your Risks
This is by far the biggest question I’ve gotten so far. Though some bodies are urging people to not buy masks and other personal protective equipment for the flu, mainly for supply chain reasons (practices in Australia are running low on supplies right now!), the evidence on whether or not coronavirus (or any virus for that matter), can be reduced in its transmission by things like masks or hand hygiene isn’t clear. There are several studies showing that transmission does go down with use of a more robust n-95 masks in healthcare workers who see this disease everyday. Medical masks aren’t shown to significantly improve rates of infection, but both treatment groups (those instructed to use hang hygiene, and those instructed to use hand hygiene and a mask) did see a reduction in rates of influenza compared to controls (yes, this was a highly reliable RCT, the only one I could find on this topic online). The facemask + hand hygiene group saw a 43% reduction vs 8% compared to controls with face masks alone, and none of the results were significant. But despite not reaching such large number, that same study ultimately concluded that these measures may help reduce rates of transmission, and that it should be recommended in crowded places during flu seasons.
Another study showed that in household studies, donning a mask, while also educating participants on the importance of handwashing, did reduce rates of catching illness by 67%. Most studies have shown limited benefits in either methods, but most studied also involved using various kinds of masks or hand hygiene after someone else developed symptoms, which may not be viable in diseases with longer incubation periods, which COVID-19 is looking like it will be (mean incubation period is 6.4 days from Wuhan epicentre case study analysis vs 2 days for most influenza strains).
Does that mean you need one if there’s no evidence of a major pandemic in your area? No. As there seems to be a global shortage – let those who need it most – healthcare workers who may be screening for this now – get their supply first if you’re well. But if you are a cancer patient, someone who’s got those comorbidities listed above (cardiovascular disease, chronic lung disease, diabetes or hypertension), I wouldn’t blame you for being cautious – especially if you’re going to hospital!
Finding a Cure
Another concern is media misinformation, and misinformation being spread by people on Facebook trying to make a quick buck off this epidemic. From that example of someone trying to sell bleach, to things you’ll see often in Twitter, or Facebook Groups everywhere, no – there is no verifiable cure for coronavirus yet. Research hasn’t demonstrated the virus is liekly to be susceptible to Tamiflu yet, but if you’re getting symptoms, and your doctor recommends it – take it. Though it may not be the easiest pill to swallow, it’s most effective taken soon after infection, and you could well have the flu which can be mitigated in its severity with Tamiflu!
Several homeopathic remedies have been suggested and are being sold to people on Twitter and in Facebook groups – don’t be fooled by the name. If it’s not being prescribed by a doctor, it likely won’t work, and you spreading that it could, could lead to people not getting seen by doctors, being diagnosed and properly quarantining themselves for one. Be very careful with what you say online!
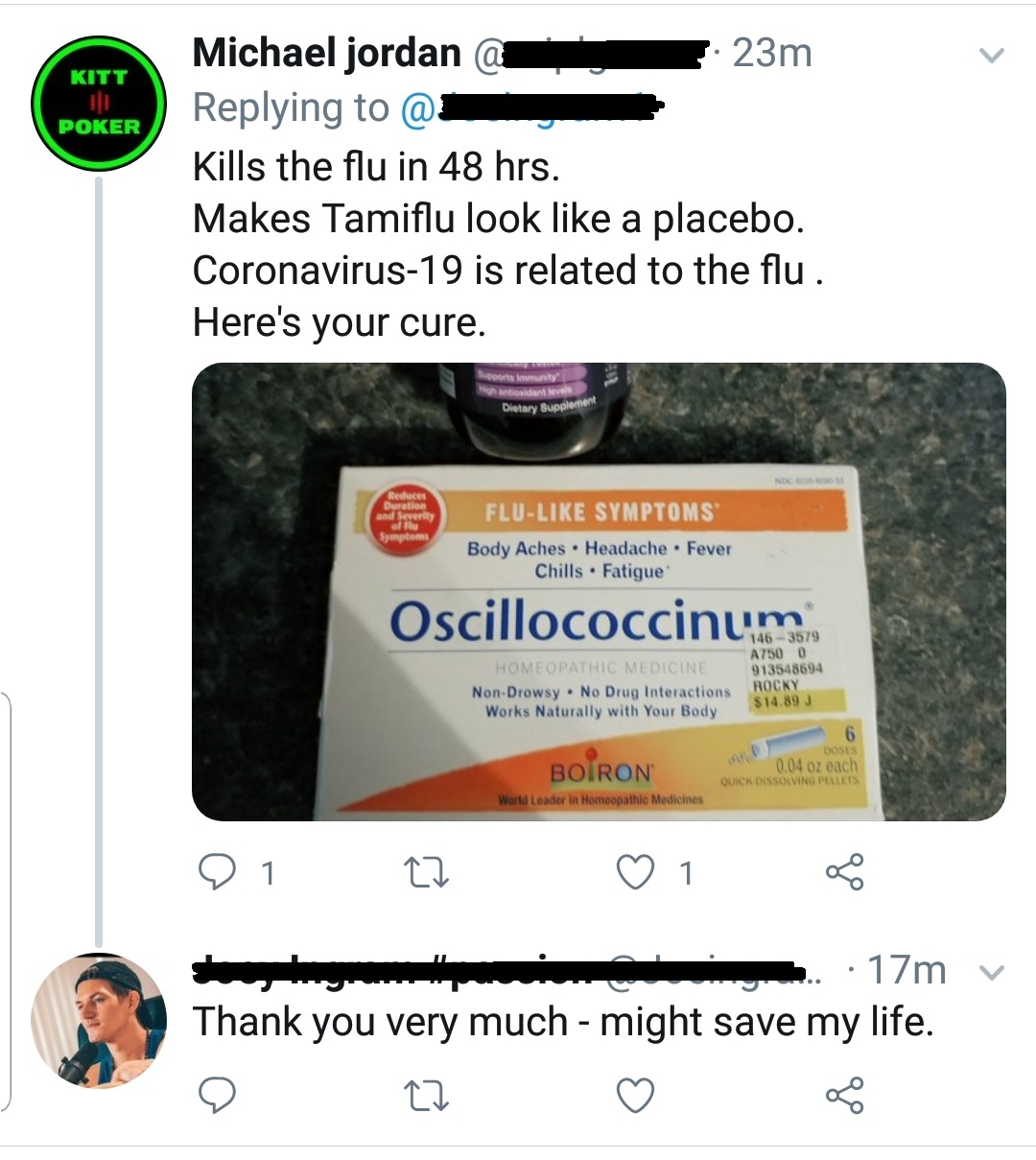
Does Tamiflu work on it? Right now – there’s no evidence for it, so this piece of information is pretty damn crap as there is no “placebo”. But oscillococcinum, though deceptive packaging (not to mention the confusing name) may suggest otherwise, is homeopathic, and thus, ineffective. Its development was based on the idea that influenza is caused by a strain of bacteria. It is not.
Vaccines and antivirals vs COVID-19
In terms of vaccines, the world is responding rapidly. I saw my doctor on March 6, 2020, and he informed me there were 2 phase 1 studies going on, already, for the coronavirus vaccine. While it may not be included in the flu shot for Australia this year, it almost definitely would by next year. Phase 1 studies are occurring around the world. This one is estimated to be completed by September 2020, this one will start recruiting soon, and this phase 1/2 study will be recruiting soon as well. Several antivirals, including remdesivir, which was developed to combat the ebola virus, are also undergoing clinical trials.
Will the flu shot save me from getting COVID-19?
Donald Trump was recently reported to have asked why the seasonal influenza vaccine couldn’t be used to stop coronavirus transmission. Vaccines are targeted towards activating your adaptive, target-specific immune system. Basically, this response by your immune system relies on training, and facilitating the spread and growth of killer cells and ‘antibodies’ that respond to a particular, disease specific target. So vaccines targeting certain strains of influenza won’t result in cells that kill the COVID-19 strain of coronavirus. But in having said that, my doctor recommended I get the flu shot to reduce my chances of getting the coronavirus, as doctors are in my local health district. Why? Because, through various mechanisms, such as the release of factors which suppress immune responses, or the killing of cells which normally would block infections from taking hold through various mechanisms too. This study modeled the potential for flu vaccines to prevent SARS outbreaks through the reduction of influenza in hospitals, where these diseases tend to spread most, and spread most severely. We know that the flu, likely most severe viruses for that matter, diminishes your immune system and makes you more susceptible to secondary infections. Though these are usually bacterial, it is very much possible, especially when there are numerous strains of diseases with very different genomic profiles (making it less likely T cells that may have developed in response to one infection could eliminate a secondary infection with another disease), as is the case with seasonal influenza and coronavirus coinciding, for viral infections to occur after having had another. So make sure you get your flu shot people!
Another curious issue is the name of the disease. Thus far, the disease itself has been named COVID-19, and the international Committee on Taxinomy of Viruses is calling the virus itself SARS-COV-2. The WHO and this committee put out their naming declaration on the same day. The only actually published announcement I could find on “SARS-COV-2” was in a non peer reviewed journal, making me feel some researchers wanted to jump the gun and get a name for it first, But considering the impact SARS had in Asia about a decade ago, the fear it entails, and the propensity for this to be blown out of proportion by media outlets, given the previous SARS epidemic had a much higher 9.4% mortality rate, the WHO recommends using COVID-19 when talking about this – which is what I’ve done throughout this piece.
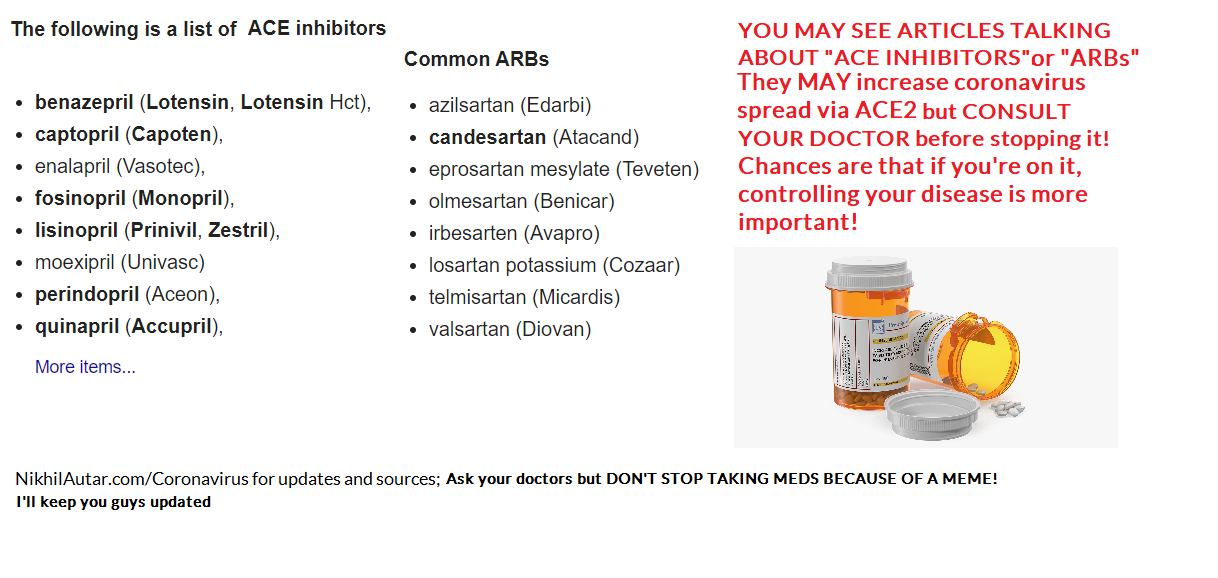
I saw something about ACE Inhibitors or ARBs (common heart drugs) being dangerous. Should I stop them?
But THIS IS JUST A STUDY and indeed a hypothesis for now. The study itself highlights the fact that there needs to be further investigation into this. Stopping ACE inhibitors and ARBs cold turkey will definitely make you feel crap and could possibly lead to more severe side effects or disease outcomes, depending on what you’re taking it for. So don’t do this
Is it a disease that only affects the elderly?
It’s true, as I outlined above, that elderly people do suffer most, and comprise the vast majority of deaths due to COVID-19. But not only is there a chance of young people dying to it too, as is being seen around the world, numbers from the CDC suggest that young people are not spared suffering. 12% of ICU patients are 20-44, 20% of people in hospital with it are in that age group too. 9% of deaths occur in the under 65 age group. None of this is insignificant. As I outline here, ICU is one of the most traumatizing things. And there are numerous reports of permanent lung fibrosis, or scarring, occurring too.
Can Children (and Anyone for that matter) get Permanent Lung Damage?
Early on in this virus, doctors were making claims that fibrosis was evidence in the lungs of patients with COVID-19. Fibrosis is a scarring element that is permanent.
These radiological findings have been confirmed, as seen in this medical journal of Australia review of sorts, which suggests up to 17% of severely ill, critical patients have evidence of fibrosis. A 15 year follow up of SARS coronavirus patients also confirmed that as many as 4.6% of a mostly healthy population had decreased lung function after their infection. Some health bodies are suggesting that this isn’t progressive fibrosis, which is good news in that it is not likely to cause long term inflammation in the lungs, but permanent disability and lung function is demonstrated through previous coronavirus outbreaks’ data, and through studies on radiological findings of the current pandemic – which suggests as many as 17% of severely ill patients are demonstrating signs of fibrosis (this number are likely to rise on follow up). It should also be mentioned that that Pulmonary Fibrosis Foundation is a press release, not a paper. It could be worse.
Children, though less likely to suffer from severe illness, are being admitted to ICUs in 0.58-2% of cases, according to CDC numbers in the US, and the most comprehensive study on paediatric outcomes out of China. It’s also evident that infants under 1 are at significantly higher risk of ICU admission (4x that of other children), and thus, exposure to this permanent damage. Not only is this linked to permanent lung damage, ICU admission causes severe trauma and PTSD too.
It is concerning to see that sending children back to school is being encouraged by governments around Australia, against medical consensus which suggests otherwise. Young people are similarly being asked to sacrifice themselves to attain herd immunity, but not only are there much higher rates of ICU admission and deaths being seen in 20-44 year old age groups when hospitals are overwhelmed, long term deleterious side effects of this through things like lung fibrosis is likely, and could have even worse economic outcomes in the long run too. Finally, sports leagues around the world, including our NRL, are also thinking about opening back up. With athletes in particular set to be severely impacted by lung damage, this should be taken into consideration too.
It’s not to say we shouldn’t reopen. But we should definitely not be looking to infect people to attain ‘herd immunity,’ not only because we’re not sure that proper forms of immunity will mount after infection (as opposed to vaccines which are optimized to create lasting infection – something I can explain further as a tumor immunology researcher), but because it could be much more dangerous than we imagine.
As someone who does have permanent lung damage of some kind due to chemo treatment, trust me, this is not something you want. I don’t know if I’ll ever be able to run again, yet alone do things like play basketball. You do NOT want this for your kids.
#DontRiskYourKids
What can you do to help?
Well the most effective organisation I could find, as judged by GiveWell and Charity Navigator (the number 1 and 2 evaluators of charities out there), is Direct Relief which is working with Chinese organisations and in the US and Carribean (and other places) to deliver money for research and PPE (personal protective equipment). That’s one way you can help.
Another way you can help is by Giving BLOOD! There is ALWAYS an outcry for more blood donations come influenza season, and blood banks around the world are doing the same.
Finally – the fact that there’s only been 1 study ever done on the impact of masks and hand hygiene on viral transmission rates globally irks me. My startup Centered Around You not only provides evidence based, AI powered wellness advice for the first time to general consumers, but also collects data in research friendly ways. Indeed, we have the potential to conduct a prospective follow up study, and more on this very task. Sign up for our email list to be kept aware of updates to this and to help aid research in this field.
And sign up to my email list to get updates on everything coronavirus and on other, mostly, health related stuff! I’m an ex cancer patient, current medical student, tumor vaccine researcher and founder of a few startups (to name a few things I do). I’d love to hear from you too! So check out my Facebook, YouTube, and Instagram if you’re there too!
]]>
I should have noticed the red flags as soon as I saw that ridiculous logo and huge picture. I mean who starts a blog post off with a large, centred picture of some generic image, right?
When you dig deeper into articles that make bold claims like this though, you often will come across big issues.
This article cited just one medical journal article, which claimed “93% of patients would prefer cannabis to other drugs”, and that “81% of patients reported cannabis alone being better than combining cannabis with opioids” – those high numbers alone instantly screamed “red flags” to me. But upon deeper inspection, there were several more flaws in the study (linked here)
.
First off, a survey study, with no mention of HOW patients were recruited, any randomisation or other such checks or balances or ways of reducing bias destroys the reliability of such a survey completely. This could have (perhaps, it likely was) distributed through a series of pro cannabis pain groups on Facebook for all we know – which would obviously make all results biased.
There are validated pain scales, and better ways of studying the effects of treatments like this, like prospective follow up studies (if not RCTs) of patients who tried cannabis versus those who tried opioids. Though these are harder and more expensive to conduct, if doing a self reported outcome studies – which can still be quite valid (though it’s hard to do this when retrospective) – the authors could have used many techniques to make their findings more solid. They didn’t.
And though the journal this article was published in is peer reviewed, its CiteScore (similar to journal impact factor) is 3.1 – which is quite low – and definitely guilty of publication bias from the quick inspection I did of its most recent titles.
And to boot – I didn’t see much evidence that legalised cannabis is actually responsible for the crippling of opioid sales so much as government crackdowns on opioids. When PROJECTIONS put total displacement of pharmaceutical sales at just $5bn, when the top 15 pharmaeuticals alone generate $560bn in revenues every year, that’s hardly a ‘huge pinch.’ ESPECIALLY when you consider that most applications of medicinal cannabis in patients can and are being patented. Including in pain.
Cannabis is an interesting drug. It DEFINITELY has amazing impacts and potential to help A LOT of people out, likely with less side effects and more efficacy than current treatments for sure! But it also has a cult-like following of #woopedallers who overblow its ability to cure ANYTHING AND EVERYTHING just because it’s #NATURAL and #DANK too.
I did a quick literature review of the matter, going into it thinking, if anything, that medicinal cannabis’s most commonly studied compounds, CBD (cannabidiol, a non psychoactive compound that acts on cannabinoid receptors in the body), and THC (a psychoactive compound that also works on those receptors – a summary of the endocannabinoid system is shown below), would help in chronic pain with minimal side effects – or at least not be harmful. A general view held by many (not just potheads, but doctors as well) is that MJ is not too harmful. But the results were surprising. To summarise, it seems THC, the main compound used to treat chronic pain, seems to make pain more bearable in some, but given its ability to cause mainly psychiatric side effects (including exacerbation of pain, the very thing we’re trying to treat, anxiety, and the activation of psychoses), caution and further research must be done to validate its use, and use cases.
In chronic pain – this great review – reviews are high quality, reliable studies, as they gather data from numerous great sources, goes into the fact that compared to opioids, cannabis based pain treatments actually caused more side effects than opioids per person treated with a number needed to harm as low as FIVE in patients being treated with cognitive issues – https://academic.oup.com/painmedicine/article/10/8/1353/1857926 – while showing no evidence of superiority to opioids either.
This study actually showed cannabis made chronic pain WORSE in most people who got them – AND higher risk of anxiety too! They didn’t even reduce opioid use.
This is in addition to the other, downplayed risks associated with chronic marijuana usage. For instance, smoking cannabis leads to a 76% higher chance of you developing lung cancer. Addiction IS possible, as is tolerance and dependence, and the latter (dependence = the experience of withdrawal when stopping a substance) is experienced by as many as 4.3% of Americans at one point in their life. As many as 3/10 Americans who’ve used marijuana will develop dependence to it, (that number rises to 4/10 of high risk youth), DSM-5 criteria (official psychiatric disorder diagnoses essentially), which added cravings and withdrawal to criteria to determine someone has “cannabis use disorder,” 19% of regular lifetime users will have SEVERE addiction, and 48% of those addicted are not functioning in ANY major role. 7.4% of American youth are abusing cannabis or dependent on it.
Contrary to popular opinion, you do develop withdrawal symptoms when coming off marijuana (dependence) – with patients experiencing symptoms 24-48 hours out of cessation (it can last up to 3 weeks, but usually is bad for a week). Though not as addictive as other drugs, it can indeed induce cravings too (addiction).
Despite claims it’s “100% safe” and that it “never kills anyone due to overdose ” (deaths due to overdose are indeed very hard to induce via cannabis), almost 350,000 people enter EDs every year because of it for various reasons (anxiety/panic to seeking help for addiction – which accounts for over half of these – 177,000 incidences per year).
All reviews and rigorous studies point to the same thing – that cannabis could help in SOME patients with chronic pain (eg this review shows that patients with neurogenic pain could benefit ), but that they DO have harms, and aren’t as efficacious to general populations as people believe. Some suggest that CBD – cannabidiol – one of the major MJ-derived compounds used for medicinal purposes – which has a much lower side effect profile compared to THC (the other major MJ-derived compound studied for medical purposes. It’s the psychoactive component that causes you to get “high”), may improve pain, particularly neuropathic pain, without much in the way of side effects. But THC is the substance most studied in chronic pain thus far, which does have significant side effects.
ALL reviews ask for more rigorous studies on the matter. Studies can’t even agree if increased THC:CBD ratios increase or decrease pain – some suggest that CBD decreases the impact of THC on pain while others say the opposite. Similarly, given up to 10% of people with migraines use it for pain relief, and that there is evidence of it helping out in a subset of these patients (likely mostly those with centrally derived pain), and that we don’t understand the mechanisms and effects of the development of tolerance (if we knew how quick tolerance developed, we could possibly help guide patients in getting maximum benefits for as long as possible while on cannabis) – we NEED to study this potentially wonderful treatment. In a similar trend we see in the literature, we NEED to do more research on this. An interesting way we can do this is through medical apps – indeed, I’m creating one which looks into gauging the efficacy of wellness interventions – and this study done by a company named StainPrint, demonstrated that migraine patients, 50% of the time, get pain relief from medicinal marijuana, but that tolerance develops in time.
Sign up to not just help power medical research, but also to get a chance to win awesome free stuff!
Overall – Medical Marijuana is likely not a viable first line treatment option that we should be prescribing for pain patients in favour of other, less harmful treatments, like cognitive behavioral therapy, treating causes of pain and other neuropathic/antidepressant/medication based treatments. Opioids may help some who don’t develop tolerance better too.
But that isn’t to say opioids, or #bigpharma are amazing either. The opioid epidemic is VERY real and a direct consequence of a few pharmaceuticals going borderlinie LEGALLY rogue (though often going illegal too in its marketing practices) and making wild claims about their drugs being safe and effective. Corrupt and/or negligent doctors WERE very much part of why this got out of hand and has resulted in mass spikes in opioid related deaths in America and other developed nations too. John Oliver explains this REALLY well in this piece – but when a system exists where a single family can PROFIT despite paying billions in fines and breaking criminal law, and killing half a million people in the process… that’s just as bad as snake oils salesmen scamming people and taking lives in their own insidious way too. 1/32 people prescribed 200mg equivalents of opioids DIED during this overly salacious period of prescription https://www.ncbi.nlm.nih.gov/pubmed/26977701. And today, as the government bears down on prescribing these drugs arguably too heavily (denying legitimate patients who NEED these drugs to function), even more are dying to things like suicide.
Lack of phaemaceutical oversight is something I’ll be calling out too – even if it loses me fans – because that too is wrong. There is no reason pharmaceuticals should be allowed to use the tactics they are allowed to. Right now, they spend more than TRIPLE on selling drugs than they do developing new ones. Drug development is skewed too much towards profit these days and productivity/innovation is going down as less and less drugs are in the pipeline – it does need fixing.
I actually wrote a paper on this which never ended up getting published anywhere but did still place me highly in a national essay competition. You can check that out here –> https://nikhilautar.com/improvingbigpharma/
But another downside of opioids is its potential to be addictive, for patients to develop tolerance and/or withdrawal too. This is often overlooked by doctors. I talked about my own experiences of dealing with this recently on my Facebook page – which you can check out by clicking here!
Big Pharma Losing Money As Patients Switch From Opioids To Cannabis
]]>
Before I did, I figured, I better bring this to people’s attention. As a medical device founder, and ex cancer/chronic illness patient, I figured I was one of the best people to do so.
As I explain in this video, right now, Facebook is MANUALLY APPROVING ADs that are illegal by several jurisdictions. One example, a page and facility named VeritaLife, sells cancer patients false, unproven remedies and markets them as cures, targeting cancer patients in the process. They not only make medical claims without medical device/drug approval (yet alone a shred of clinical evidence) – they also do other illegal things, like using testimonials to market medical interventions.
As I explain here, in this article on how these people nearly convinced me to forgo therapy for alternatives – people who even try alternative treatments have a 2 – 5.7x higher chance of death. They’re more likely to avoid surgery, radiation or chemotherapy (7%, 54% and 34% more likely respectively), which leads to these higher rates of death. These people are even more likely, as they will almost ALWAYS avoid proper, proven therapies. There are NUMEROUS examples of GoFundMes sending people to Mexican/Thai/other clinics, that require tens to hundreds of thousands (which is direct profit to these clinics’ bottom lines) – as seen in the video and below.
This could be occurring because they’re located in different jurisdictions. But when advertising to Australia or the United States, I know you need to abide by local ones.
This is just the tip of the iceberg. There are several similar ads that also toe, or step over the line, when it comes to medical device and wellness marketing that Facebook is getting wrong too (I provide some examples below).
If you see a dodgy ad, you can report it to your local medical regulator, or advertising commission. Here’s a link to the TGA’s one for Australians, the FDA has a complaint process too which can be found here. Feel free to send anything dodgy you see to my Facebook page, or directly to my email info at nikhilautar.com or at www.nikhilautar.com/contact . I’ll compile a list of this. Hopefully together, we can stop this crap.
The fact that Facebook is profiting off this COULD make them liable. Their advertising policies do ban some things (though, as you’ll see below, things do fall through the cracks) such as MLMs, which often lead to dubious health claims, as well as financially drain vulnerable populations. But there are several . So be sure to sign this petition and share it too – hopefully we can make an impact. http://chng.it/n8qQjtVyZb
Here are a few more examples of this nonsense with proof. In that video, I show you how to report and ad to Facebook – which is also a useful way of making change.
Blacklisted sites can still advertise on Facebook.


You can’t find The Truth About Cancer on Google, because it’s either blacklisted, or had traffic diverted due to its promotion of non proven therapies. Yet Facebook approves ads for them.
Toeing the line. Dubious, perhaps illegal marketing making health claims at the very least scam, at the most, target vulnerable populations.

This company sells weighted blankets. They usually comply by laws, but as seen in the final ad, their claim that weighted blankets “reduce stress, anxiety and improve sleep” could be in violation of laws. They don’t have proof to back this up, and aren’t a registered medical device, but give the impression that they are by doing so.

Faceobok pages are VERY effective marketing tools. “Lookalike” audiences target people most likely to want your product. A weighted blanket company uses another page’s profile to sell their weighted blankets. This practice isn’t illegal. But this ad, like the last panel/ad highlighted in red above, did also make the claim, WITHOUT “MAY” or DISCLAIMERS that weighted blankets reduce stress and anxiety.
This isn’t as severe as companies like The Truth About Cancer or Verita Life, as it isn’t targeting people at immediate risk of death. But making false claims can make people with depression and anxiety suffer more. Not to mention, ‘scamming’ these populations and putting them under financial stress is NOT an ethical move.
MLMs
Forever Living is an MLM – a “multi level marketing” scheme, which are designed to emulate pyramid schemes, but technically they aren’t as they skirt the law (many are pyramid schemes, legally, but are simply not being prosecuted). Facebook’s advertising policy prohibits them for advertising them on the site. Yet here I show one that’s either slipped through their cracks, or going on WITH their knowledge.
As seen here, they also often target stay at home mums, a HUGE demographic of people who are vulnerable to their sensationalist claims of being able to make money from home, and who fall for their cultlike practices.
Send me any dodgy ads you see or join my email list and keep up to date with what I’m doing!


And now… Verita Life
They make false medical claims without any disclaimers, and without medical device approval.

Seen a dubious page on Facebook making dodgy health claims?
Here’s how you go about reporting them.

You can find out more about a Facebook page’s ads by clicking this button.

Click this next – and you’ll start seeing the next screens – the ads that a page is currently running. As seen – you can find out WHERE they’re targeting. The previous page shows where they’re located – as does them obviously mentioning it in the post, as seen below.
. 

An excerpt from their website. They regularly make unverified health claims, but look really professional. It’s understandable how anyone can fall into their trap. They immediately try and enter you into their sales funnel, which mainly comprises representatives contacting you. As I get out of surgery, I’ll investigate this further for sure.


Examples of advertising that’s OK


Top/left – Dubious ‘coaching’ clinics promoting alternative therapies, though it’s doubtful if they work, aren’t illega.
Bottom/Right – Swisse, one of Australia’s largest vitamin manufacturers DOES comply by advertising and regulatory guidelines and almost always adds disclaimers to promoted content.
Thanks. I should be alright during this surgery. But in case I’m not, keep up the good fight!
]]>
No but seriously, this is a tactic used by gun right advocates in the US. And it works. News cycles on dramatic events obviously ramp up clicks on a topic when something occurs. Stalling at these times leads to less talk about an issue.
But in this case, that won’t really work. And you know, what. In this case, I may actually agree with people yammering on about this not being the right time to talk about these things.
Climate change is LIKELY to be behind why our bushfire seasons are getting worse. For those nerds out there, like me, who paid attention in high school geography class, yes, El Nino effects – mass changes which occur in Ocean Currents that lead to seasons of terrible drought and increased fire-risks – can affect the Eastern Coast of Australia. They occur periodically, in cycles. But right now, we’re not in an El Nino cycle. Climate change is very likely a reason why we’re currently in one of the worst fire season, despite us being in November (that’s STILL SPRING in Australia!), in decades.
But right now, we’re getting people talking about climate change constantly. Protests are helping do that, for sure. But this, in an emergency, where news is rightly focusing on updating people on fires, and how to stay safe, and in an issue which isn’t as obviously caused by an issue to most reasonable people’s eyes, may not be the best time to talk about it.
But also right now, politicians are racing to see who can grab the most attention out of this. People have been blaming the Greens (a left leaning environmentalist party) for not supporting backburning, a practice where you deprive potential future fires of fuel by controlled burning of bush brush. That’s not true. And though I’d say it’s a stretch for a Greens senator to retaliate by calling coalition politicians “arsonists,” what ex power-broker of the right-leaning coalition party, Barnaby Joyce said next went WAY too far.

2 people died in fires yesterday. And this person, who was once in the running to be our PM, insinuated that their political affiliation led to their death.
HOW THE HELL IS THIS EVER OKAY TO SAY?
Why is THIS not something that should ever be said?
What are your thoughts on the matter? I’d love to know. Check out my other satirical posts/stories of funny things that kept me smiling during hospital. And yeah, if you’d actually like to join that email list to get word of my next post – you can do so here.
]]>
True struggles were finally outed for embattled Inner-western suburbs university student and influencer, Ketchup Sharmautar, as he opened up to his month long struggle to find anything ridiculous, yet natural, to post about trying to his 13,222 followers.
“It’s not easy being me.” confessed Ketchup, “And it’s not like you can just make these up. Getting the correct balance between something left-field enough to capture attention, while still being natural enough and marketable to make a decent margin through my online store.”
“The gold rush is over. The Good Old days of Urine Smoothies and Coffee Enemas are gone. You just can’t be original without risking organ failure these days.” He sighs.
When asked why he didn’t just promote good, healthy advice, Keshav had this to say. “You try selling people evidence-based advice. It’s boring. Like and follower suicide.”
While it is true that the best weight loss solutions involve a bit of work and conscious control of some dietary habits, the explosion of Instagram Stars online has fueled more and more misinformation. Cancer Researcher Nikhil Autar points out that cancer patients who took alternative medicines have a 2 – 5.7x higher rate according to numerous studies, with various factors to blame. But you don’t care about those peer-reviewed sources! Read on!

“This used to work wonders, until every single combination literally ran out. How am I supposed to get validation from my friends on Facebook now? To share the official Complimentary Medicine Organisation generator, or to comment your own natural therapy – click here.
“I tried everything. From picking through compost mounds and pulling out random combinations of fruits and veg, to using Alternative Medicine Generators, nothing worked!” exclaims embattled 24 year old star, Ketchup. “Since my amazing vitamin company that I’m-not-allowed-to-say-the-name-of-in-public-but-am-allowed-to-if-you-DM-me went belly up, I’ve actually considered selling pharmaceutical products on Instagram.”
“I don’t have an obvious disability or anything. Apparently pharmaceuticals have enough ethics to insist on that.” scoffed the little prick, while examining his hairline on his phone’s front-lens camera. “But I’m sure I could pull a Gibson on people and call it a prank.” he laughed.

Instafamous Entrepreneur, Ketchup, Pictured here, understandably disappointed by an eggless sugarless cake he was forced to plug during birthday celebrations.
“You know how hard it is to get alternative cake that’s Vegan, Gluten and GMO free AND Organic these days??? Of course it tasted shit.”
Pharmaceuticals are actually selling real medicines via Instagram in a desperate bid to reduce sales budgets, which now are greater than 3x R&D spend. “We saw the amazing successes of completely made up things… We figured our actually proven stuff would sell like hotcakes.
Influencers are conflicted, however. “I’m not sure if something shown to work can be alternative enough to match our audiences.” pouts 80% of all Instagram models selling you a juice cleanse. “I mean I LOVE the fact that they cost followers thousands, as that generates large profits from me. But the whole ‘proven to be safe and effective through numerous clinical trial things’ doesn’t really sell as much as you think it does.”
This has not been Nikhil Autar (not the Nikhil Autar who was interviewed before, or who’s in the URL of this article), I swear, and you should definitely NOT subscribe to his infrequent email list if you approve of alternative medicines being able to make whatever claims they want. PS – next time, I talk to another legit Instagram Influencer who insists his pyramid scheme shaped business is actually just a triangle on this episode of #MedicalFactz
[email-subscribers namefield=”YES” desc=”” group=”Public”]
If you wanna learn about that time that I was almost killed by misinformation spread by a guy trying to sell me supervitamins from his “Not a pyramid scheme because pyramid schemes are illegal and we’re still being prosecuted right now” multi-level marketing company – click here.
To lend your voice against social media stars/alternative medicine practitioners who DON’T MAKE DISCLAIMERS THAT WHAT THEY SAY OR DO IS NOT MEDICALLY PROVEN OR SHOWN – something they legally should be doing – click here. If you wanna tweet about the change.org campaign – click here.
Click here if you wanna tweet this article to your followers!

I wanna make it sure this is absolutely clear, this is NOT Nikhil Autar who wrote this and you should NOT check out his Instagram or social media accounts – @nikhilautar .
And you should DEFINITELY NOT listen to what he says just because he’s a researcher and is pictured in a lab coat in a certified lab. Because even he’d say to fact check EVERYTHING you see via credible sources!
]]>I recently went on CoffeZilla’s podcast today, and outlined a few experiences I had with dodgy MLMers and alternative clinics who advertise on Facebook, netting them millions, and Facebook tens to hundreds of thousands. Here’s a bunch of evidence and screenshots of other conversations I’ve had with scammers/MLM grifters. It’s REALLY sad to see.
For those who don’t know me… My name is Nikhil. I’m a medical researcher, medical student, and ex cancer patient.
I’ve been on both sides of the medical bed in my role as a patient, future doctor, and have also been in the background too – working on, and advocating for medical research. Again, in both my capacities as a professional AND a ‘consumer.’
I’ve looked up the literature, evaluated trials and fought to get the medicine which has probably kept me here (azacitidine, which was in early phase trials for my condition, when I’d relapsed, and needed it most). I’ve also been on numerous alternative therapies, from low sugar diets and alkaline water, to tumeric, Chinese herbs, and even medical marijuana. Both for cancer, and the resultant chronic, and potentially fatal illness my treatment has left me with (graft versus host disease).
I know what it’s like to be desperate. I know how crappy doctors can be when considering you as a COMPLETE patient, and person – and why and how complimentary medicine DOES make a difference. Indeed – a massage therapist, and dietician have changed my life. I’m on COQ10, Fish oil and am involved in other complimentary medicine too. Indeed – UpToDate, a tool pretty much every doctor uses every day to guide treatment actually recommends these two as first line therapy for lipid and cholesterol control.
But I also know the importance of medical science. I also know numerous friends who’ve been turned away from options which gave them a chance, and ended up dying. And in this post, you’ll read a story of HOW I MYSELF WAS ALMOST CONNED into trying Sodium Bicarbonate instead of real medicine when I’d relapsed, and given a 10% chance of surviving, and why we need to PROSECUTE PEOPLE WHO SPREAD MISINFORMATION FOR PROFIT – OR WITHOUT DISCLAIMERS (Click here to lend your voice to the the Change.Org campaign now)
Alternative medicine can be amazing. Many, if not most medical therapies DID come from nature, and knowledge of traditional medicine. And I’d say the majority of naturopaths, massage therapists and yoga teachers only encourage you to be more healthy, mindful individuals.
But especially today, where memes on the internet are unquestioned truth, whilst scientific articles and doctors are doubted (and routinely made to be subjects of conspiracy theories), alternative medicine can be dangerous. The following examples may shock you. But it happens all the time. And it’s literally killing people. Cancer patients who use alternative medicine as opposed to proven therapies have up to a 5.7x higher chance of death!
A video from my series – Medical Factz – that outlines the ridiculous “Cancer is a Fungus, and sodium bicarbonate is the cure” theory that started from fraud, and ended in jailtime for manslaughter, and millions of others being deceived.

Recently, Facebook took action after a natural birth Facebook Group urged an endangered patient to not seek medical treatment at a hospital. The baby passed away.


Right: Another pernicious danger seen often in Facebook groups… Toby is a juice advocate who sells juicing guides and products. He has no clue what cystic fibrosis is. Yet he is still trying to scam them to make a few Dollars. It’s sickening. Vertex is a pharmaceutical company who’s creating treatment for CF, by the way.
Left: One of the biggest proponents of unproven lies about health has to be the antivaccination movement. Find out how one man fraudulently wrote one paper (composed of made up patients and made up results) which caused this movement to go, pardon the pun, viral (he now speaks at conferences for tens, to hundreds of thousands).
This is just the tip of the iceberg. From treating children who contract various illnesses with essential oils and tumeric rather than getting them medical attention, to misleading desperate cancer patients with promises of miracle cures (something which has killed at least 2 friends of mine, to date), to prescribing natural therapy regimes which have left babies malnourished, likely suffering from developmental delays for life, we seem to hear about things going wrong for people every day these days.
How I was nearly killed by bad advice.
The picture below outlines a scam I almost fell for. When I’d relapsed, I was given a less than 10% chance of surviving. Palliative care was suggested as an option for me. A second bone marrow transplant was a long-shot, but the only curative option.
At this time, a family friend put my family in contact with a researcher and scientist named Dr J, who promised to have a cure for me.
I was desperate. Willing to try anything. But luckily, I also had a year of medical knowledge under my belt.
We went in to see ‘Dr’ J one day at his apartment. He went into this theory of how sodium bicarbonate could cure cancer. One common, popular alternative therapy promoted by many, is the idea that “cancer thrives in acid, and therefore making yourself more alkaline will cure it”. He also purported another common alternative therapy – that “cancer loves, and is fueled by glucose, therefore low-sugar diets will cure it.” The former is largely known to be false. Cancers, due to their rapid, anaerobic metabolism of energy emit large amounts of lactic acid which PRODUCE an acidic environment. Not the other way around. And in any case – ‘alkaline diets’ or alkaline water will only result in less acidic urine, and slightly more alkaline saliva (not associated with alkaline blood). Your body’s buffer systems keep your blood’s pH in a 0.1 window. Even 0.01 higher or lower than normal ranges result in medical emergency. There’s no way for alkalinity to make it TO the cancer.
When I asked him about how you could make tumor sites more alkaline… he had no response. And when I asked him a basic metabolism question any 1st year student in any health degree would understand (‘if cancer feeds off glucose… your body will produce glucose from elsewhere by breaking down fats and protein if need be. Why wouldn’t the cancer just keep using that glucose preferrentially?)… he again, couldn’t answer me.
He showed me a few case studies from decades ago of 1 or 2 people who seemed to have had tumours regress after trying sodium bicarbonate. But even then I’d been reading on spontaneous regressions, and even then, I knew that if only a few case studies could be produced in the decades since we had this ‘common knowledge’ of how to cure cancer… then it was unlikely to be representative, or statistically significant. And after all this, he turned his attention towards my parents and started his sales pitch on why “Amway vitamins” could cure me. Again, no clear linkages as to why his vitamins were better (or why vitamins could cure cancer for that matter) were made. I later found out that Amway is a company with a pyramid-scheme model, designed to make money through the perpetual, impossible, addition of members who go on to onsell product, and earn commissions on all members they bring into the program. “Dr” J was probably locked in this trap himself.
John Oliver, in his brilliant style, breaks down the fraud that is the many mutli-level marketing companies that exist worldwide.
Family and friends pressured me down his pathway. They said it couldn’t hurt. They told me to believe in him. They took me to a seminar where he waxed on and on, and brought up people with chronic conditions cured by his miracle therapies (when likely, their changed lifestyle habits were the real fix), where he wanted me to speak, to endorse his treatments.

I didn’t.
If he, a scientist working at the University of Sydney, couldn’t answer the questions of a 1st year medical student, why should I believe him?
Instead, I went out and looked up every journal I could, and every clinical trial going on in my disease around the world (something easier to do than expected – thanks to this amazing site that anyone can use called ClinicalTrials.gov) – I looked through all my options and presented one – Azacitidine – as a promising option to use to increase my odds post transplant to my doctor. With my doctor’s help, I got it.
It’s likely because of that drug, and hundreds of thousands of hours of work from scientists, and doctors around the world, that I’m still here today.
Yet, if I hadn’t had the knowledge I did, “Dr” J above could have killed me.
If you’re in a similar position – but don’t have medical training, please, PLEASE do a simple search on ClinicalTrials.Gov and/or your national clinical trial database for options. When I was looking up my own therapy – it helped me see trends of new therapies and backed my case to my doctor to get me the drug I needed. It’s simple to use – I’ve suggested it to numerous patients who’ve found second options and benefited from REAL SCIENCE through this. Please – try this first!
So why does this happen? Isn’t it illegal?
Consumer law protection exists for this kind of stuff. Yet misinformation like the above is rife within the multi-billion dollar alternative medical industry. You can’t sell TVs or Fridges based off false statements and claims. But somehow, it’s OK to gamble with other peoples’ lives, in health.
Why? Well, I’m not a lawyer. I’d love to hear from any medical malpractice lawyers out there who’d like to offer their own perspectives. But one major issue is that legislation against this kind of thing, around the world often lacks teeth.
This great article discussing the UK’s Consumer Protection from Unfair Trading Regulations 2008 in regards to alternative medicine – goes into some of the issues. Interpretations of the law are often not as clear as their intentions, in the eyes of lawyers and judges. Though it seemingly is clear that the defendent, not accuser, has to prove the claims they make are true, in practice, it often is up to the accuser to prove something’s false. Proving a negative is very difficult. And in a field where not much research is done… this becomes tougher. In addition, a lot of the time, enforcement isn’t followed up on laws. The Competition and Consumer Act 2010 (Australia), and numerous precedents and investigations done by the FTC also mark many of these practices as illegal.
Yet millions get away with this. Indeed, social media and fake news is a big proponent of this too. There are thousands of influencers with millions of followers making millions of dollars pedaling misleading, and often dangerous misinformation. Wellness is a half a trillion dollar, largely unregulated industry. Chinese Medicine, which I tried, were found to have 127 different types of fungal contaminants in just 15 herbal mixes. And innocuously, there are thousands, maybe hundreds of thousands, advocating for unproven therapies in Facebook groups – turning people away from real therapies – sometimes profiting, sometimes spreading misinformation. People and groups like this, I see everyday in cancer groups where I talk and interact with other patients.

A dangerous meme from a dangerous page. Mamograms are PROVEN to save lives – and their risks and benefits have been studied and found to be effective in reducing mortality in high level studies. The amount of radiation exposure is safe and though there are new therapies coming through the pipeline – Thermographs are shown to be INFERIOR to mamographs. Natural News is a notorious ‘news site’ which spreads dangerous misinformation.
Why are they never sued? Well, sometimes they are. Robert O Young, a proponent of the “cancer is acidic, and alkalysing the body is the cure” lost a lawsuit that forces him to fork over $105million to his victims. Dr Simoncini, proponent of the “cancer is a fungus and sodium bicarb is the cure” alternative theory that has been thoroughly debunked is serving a 5 year jail sentence for manslaughter, after he continued to treat people for tens of thousands of dollars a pop at his clinic, despite being convicted of manslaughter and being deregistered earlier in 2006 as well. Doctors prescribing miracle “Defeat Autism Now” therapy regimes which have no scientific basis are currently being sued too.
But often, quacks and frauds USE the law to continue shady practices. Another naturopath and proponent of the sodium bicarbonate cures cancer movement is suing a whistleblower to ensure she can keep her operation running. A senior member of the renowned site Quackwatch was also sued for defamation.
And often, this stuff goes unchecked on social media. Not just from unscrupulous people like Toby (pictured above), but also from “Influencers,” and “Wellness Gurus and Coaches” who post deliberately misleading posts to millions of followers to sell their own products, or that of other, often unproven, wellness therapies.

An example of one of Facebook’s most virulent anti-science influencer. Sure, it isn’t one of his more ludicrous posts which does things like dissuade people from getting proven, effective therapies for their serious illness, but it shows how far some of these people are willing to go to make a quick buck. Click here to check out a video I made spoofing many of those viral ‘health fact’ videos you see these days.
But you know what, I’m sick of this.
Things like this seem innocuous. But it literally kills millions every year. It scams people, many of whom are already under heavy financial strain following intense treatments, of tens of thousands. It’s taken the lives of at least 2 close friends who had other, better options still available to them, and likely many more people I’ve known too.
Alternative and complimentary medicine can be amazing. The fact that practitioners actually sit down, and take the time to listen to you as a whole person is a big reason why it’s so popular. There are many massage therapists, yoga instructors, aromatherapists, dietitians and naturopaths out there who do know their stuff, work with doctors, abide by laws – and they help DO help millions. I benefit from many of the above.
But it’s when they do things like this that they become dangerous.
I believe we need to crack down on this industry, and the crooks who lead millions astray every year. We need to #MakeAlternativesGreatAgain – and when people make false health claims – we need to #LockEmUp – for the good of society – if they make unfounded health claims. If you agree – check out this change.org campaign I’m running soon.
1) IF YOU MAKE CLAIMS PERTAINING TO HEALTH – claiming a therapy WILL cure or fix a condition, or encourage others to try such therapies, without any evidence to back up your claims, without inserting disclaimers or saying “May” – YOU SHOULD BE CULPABLE, AND YOU SHOULD GO TO JAIL if your advice ends up harming someone.
2) – If you profit from the sales, in any way, of products with purported health benefits, YOU SHOULD HAVE TO MAKE THAT CLEAR, and it SHOULD BE YOUR RESPONSIBILITY, to check the validity of those health claims.
I’ll even go so far as to say:
3) If you share misinformation, without any reasonable scientific or other evidence behind it, and it ends up harming someone – YOU SHOULD BE PROSECUTED AS WELL.
If not… scumbags like these will continue to exist, and prosper off the suffering of good people. Check out the Change.org campaign I’ve made and add your voice to this campaign for science and reason.

Bell Gibson fraudulently made millions after faking that she cured brain cancer with diet and alternative therapies. Millions of dollars escaped fines. But how many she led astray of real options will probably never be known. Full article here. She joins other fitness and wellness ‘experts,’ such as Sarah Stevenson who’ve falsely claimed they’d beaten a cancer which spontaneously regresses in over 1/4 people due to diet and wellness alone, and then gone on to fraudulently provide wellness coaching sessions, for $300 per 50 minutes (rates doctors who’ve studied for decades don’t charge).
There are numerous examples of scumbags like this out there. You may well already be following them. If you are, and you don’t see links to journals, or any kind of evidence which backs up their claim – do me a favour. Unfollow them. And if they say something which you feel may be harmful to society – tag me, @nikhilautar, or use the #LockEmUp to help bring them down.
What I’m doing about it.
I’ll be running this campaign soon, this is one thing. But my Startup – Centered Around You – actually aims to be the first app of its kind to not just provide evidence based wellness advice – but TEST IT TOO. A combination of machine learning, my own passion for research, and inputs from world leading clinicians, researchers, and coders/designers, advised by CEOs, senior VPs and heads of national operations of international and ASX listed firms advise us. We won Australian Student Startup of the Year not long ago. Along with numerous other prizes (we made the finals of the Global Impact Challenge, won NSW Student Startup of the Year in a separate competition, and have received numerous other grants and rewards for our work).
Our medical devices will also make life safer and easier for elderly and disabled patients. We are testing with some of Australia’s largest nursing home chains in the near future.
And our products have also generated interest and pre-sales from people interested in getting a better night’s sleep too!
Check out www.GetToSleepEasy and CAroundYou.com for more information.

I’m always here to talk. You can reach me (I am incredibly busy, but strive to read all my emails) at info [at [ nikhilautar.com – or via this contact form.
Wanna report a dodgy influencer who may be breaking the law?
[hubspot type=form portal=6338483 id=591a44ae-86cf-4457-a4dd-b700c0c7e181]
Common, Inaccurate Medical Claims being Bandied About Online
Check out Nikhil’s Series – Medical Factz – where he breaks down common cancer (and other health and wellbeing) trends, and finds out which are myths and which have merit!
Cancer is a fungus?
Nikhil breaks this one down below!
Vitamins cure cancer; Vitamin C Cures Cancer?
Vitamins are often claimed to be efficacious in cancer treatment when this is far from the case. SBS did a feature on this recently. A compounding pharmacist was telling patients – as A NON CLINICIAN – someone who can’t legally advise on clinical judgements according to Australian, TGA legal guidelines – claimed that Vitamin C supplements could cure cancer or help patients. The 2 largest systematic reviews – the highest quality of evidence possible – have said a LOT more evidence is required. There hasn’t been phase 3, randomised controlled trials for this. It is NOT indicated by the TGA as a treatment for cancer so even if her clinic is supported by GPs – its use is questionable and something I would be interested in reporting to authorities. Would you want big pharma skipping protocols and promoting unfounded claims before approval? No… Why should someone with NO training in this space get a pass? Multiple studies have discontinued high dose therapy use due to high toxicity. It should NOT be advocated for as a viable treatment. She did just that on national TV.
Could it help? Possibly – early studies have shown some improvement. Almost no cures. It it generally well tolerated. But toxicities have also been noted. I’ve been in a desperate position before… There are many options MUCH higher on my list of things I’d try if things got more dire.
Vitamin B6 and B12 was found in a prospective, observational study of over 77,000 patients (one of the highest quality long term therapies) have been associated with 30 – 40% higher risks of lung cancer (a 2x higher risk for patients taking high doses). Vit b12 has been shown to increase esophageal cancer as well. Many studies show no positive impact on survival. SBS – the news channel which put this together an ‘unbiased show’ where professionals with years of experience and with backing of millions of patients worth of data in research were given an equal platform to individuals who ‘just felt better’ – even reported on an American study which showed vitamin supplements increased risk of all causes of death. Indeed – vitamins nearly killed me.
How cancer patients in particular are at risk
Cancer patients who take alternative treatments are more l
Some alternative treatments also reduce the efficacy of treatments or prom0te tumour growth! For example, antioxidants may actually cause cancers to grow once established by reducing cancer-killing, toxic reactive oxidative species (ROS). Some drugs which mediate tumour cell death through inducing more ROS’s will also be less effective if you’re on a high antioxidant diet.
Wanna report a dodgy influencer who may be breaking the law?
[hubspot type=form portal=6338483 id=591a44ae-86cf-4457-a4dd-b700c0c7e181]
]]>
This was my submission to an essay competition run by the Cancer Council of Australia a few years ago. It was shortlisted but didn’t take down first place unfortunately! I was probably a bit too industry/business model focused for what they were looking for! It does outline major challenges facing drug development though – something fascinating to many, for sure! Let me know your thoughts!
Ensuring Cancer Treatments
Improve with
Advances in Research
Nikhil Autar
University of Western Sydney
Cancer Council 2015 Essay Competition
Outline
promising of prospects, and ensure our research system has maximal efficiency. In this essay, I’ll discuss the changing nature of cancer treatments and outline where and how we should direct our research to achieve maximum improvements for patients. I’ll also delve into the challenges clinical and academic research face, and suggest systemic solutions that will ensure research of all kinds are done in the most time-and-cost efficient manner. And finally, I’ll discuss the importance of preparing future physicians to deliver the fruits of research.
Epidemiological:
Increasing Incidence Due to Age
nations5,6, following improved treatments, systems, screening programs and prevention measures7,8. But overall, in the developed world, cancer incidence by type is changing slowly5. The major epidemiological change is an increase in overall cancer incidence due to an older population9-11, who, through various intracellular and extracellular processes, are more likely to develop cancer12,13. Hence research, especially clinical-trial research, should reflect lower tolerance of toxicities, higher rates of co-morbidities14, and other factors prevalent in older populations.
Biological:
The Targeted, Personalised Future
Translational: Less New
Drugs, More Expensive Research
Improving
Clinical Trial Infrastructure
Using
Technology to Reduce Time and Costs Taken to Trial.
Teamwork
Strategies That Unite Researchers From All Sectors
Strategically
Directing Basic research
require this sectors’ funding4,120,122,124. Innovative, assertive, collaborative strategies, such as the one used by Australia’s own Cure Bain Cancer Foundation, reduce wastage and increase output in this vital research stage125. The Foundation proactively outreaches to researchers when providing grants, saving over a month of work per-researcher-per-year135, collaborates, and indeed, directs research strategies for the Global Brain Exchange consortia126, and works actively with industry to ensure treatments reach patients125. Similar strategies, if employed by others, would lead to leaps-forward in treatment prospects, and thence, patient outcomes.
emperor of all maladies. New York:
Scribner; 2010.
Insitute Of Health and Wellbeing, Cancer
survival and prevalence in Australia, Period estimates from 1982 to 2010, CANCER SERIES Number 69, Cat. no. CAN 65
Medicine. Personal communication, 2014.
and Prevention, Front Oncol. 2011; 1:
3
primary cancer analyses from the Surveillance, Epidemiology, and End Results
(SEER) Program. Oncologist. 2007
Jan;12(1):20-37
2009;18:1688-1694
of Cancer, 1975-2006, featuring
Colorectal Cancer Trends and Impact of Interventions (risk factors,
screening and treatment) to reduce future rates. Cancer. 2010;116:544-573
de Vries E, Arnold M, Altsitsiadis E, Trakatelli M, Hinrichs B, Stockfleth E,
Coebergh J; EPIDERM Group. Potential
impact of interventions resulting in reduced exposure to ultraviolet (UV)
radiation (UVA and UVB) on skin cancer incidence in four European countries,
2010-2050. British
Journal of Dematology. 2012
Aug;167 Suppl 2:53-62
Institute of Health and Wellbeing, Cancer incidence projections: Australia, 2011 to 2020. Cancer Series no. 66. Cat. No.
CAN 62. Canberra: AIHW, 2012
primary cancer analyses from the Surveillance, Epidemiology, and End Results
(SEER) Program. Oncologist. 2007 Jan;12(1):20-37
L, Ershler WB, Balducci L, Ershler WB. Cancer
and ageing: a nexus at several levels. Nature
Reviews Cancer 2005;5(8):655-62.
Clin Geriatr Med 2012;28(1):1-18
Audisio RA. Principles of surgical
oncology in the elderly. Clinical
Geriatric Medicine 2012;28(1):51-71.
Impact of the Completion of the Human Genome, Toxicologic Pathology,
32(Suppl. 1):1–2, 2004 DOI: 10.1080/01926230490424987
of Cancer” Accessed 12 April
2015, accessible from: http://cancergenome.nih.gov/cancergenomics/impact
Jan H.M. Schellens
Jun; 16(6): 800–810. doi:
leukemia: focus on imatinib (Glivec®, Gleevec
 ) Journal of Therapeutic Clinical Risk Management 2008 Feb; 4(1):
) Journal of Therapeutic Clinical Risk Management 2008 Feb; 4(1):163–187.
EGFR mutation and resistance of
non-small-cell lung cancer to gefitinib. .New England Journal of Medicine 2005 Feb
24;352(8):786-92.
Derek J. Jonker, Chris J. O’Callaghan, Dongsheng Tu, Niall C. Tebbutt, R. John
SimesHaji Chalchal, Jeremy D. Shapiro, Sonia Robitaille, Timothy J. Price, Lois
Shepherd, Heather-Jane Au, Christiane Langer, Malcolm J. Moore, and John R.
Zalcberg, K-ras Mutations and
Benefit from Cetuximab in Advanced Colorectal Cancer New England Journal of Medicine 2008; 359:1757-1765October 23, 2008DOI: 10.1056/NEJMoa0804385
KRAS is required for panitumumab efficacy in patients with metastatic
colorectal cancer. Journal of Clinical Oncology. 2008
Apr 1;26(10):1626-34. doi: 10.1200/JCO.2007.14.7116. Epub 2008 Mar 3.
Lancet.2009 Mar 21;373(9668):1033-40. doi:
10.1016/S0140-6736(09)60251-8.
Group, September 27 2012,
Accessed April 12, 2015, Accessible from: https://kmrgroup.com/PressReleases/2012_09_27%20KMR%20PBF%20Success%20Rates%20by%20Molecule%20Size%20Press%20Release.pdf
biologics, PharmaTimesDigital, March
21 2012, Accessed 12 April 2015, accessible from: http://www.pharmatimes.com/article/12-03-21/Pharma_patent_filings_fall_amid_shift_to_biologics.aspx
Hughes, Antibody–drug
conjugates for cancer: poised to deliver? Nature Reviews Drug
Discovery 9, 665-667 (September
010) | doi:10.1038/nrd3270
of bacterial ghosts in biomedicine Advances in Experimental
Medical Biology 2009;655:159-70. doi: 10.1007/978-1-4419-1132-2_12.
EM; Luft JC; Bridges AS; Kuijer JL et al. “Plasma,
tumor and tissue pharmacokinetics of Docetaxel delivered via nanoparticles of
different sizes and shapes in mice bearing SKOV-3 human ovarian carcinoma
xenograft”. Nanomedicine 9 July
2013 (5): 686–93.
Cullis PR (2004). “Drug
Delivery Systems: Entering the mainstream”. Science
2004 303 (5665): 1818–1822
sensitization of human tumor cells by a novel checkpoint kinase inhibitor, AZD7762. Clinical
Cancer Research. 2010 Apr 1;16(7):2076-84. doi:
10.1158/1078-0432.CCR-09-3277. Epub 2010 Mar 16.
lung cancer. Cancer Control. 2014
Jan;21(1):80-9.
J. Old, Antibody
therapy of cancer, Nature Reviews Cancer 12, 278-287 (April
2012) | doi:10.1038/nrc3236
rituximab and beyond. Hematology, the Education Program of the
American Society of Hematology 2007:233-42.
treatment of colorectal cancer. Journal
of Clinical Pharmacy and Therapeutics 2007 Feb;32(1):1-14.
Lina Tornesello, Franco M. Buonaguro, Translating
Tumor Antigens into Cancer Vaccines, Clinical
Vaccine Immunology. 2011 Jan; 18(1): 23–34.
Vincent Magrini,
Michelle
Becker-Hapak, Saghar
Kaabinejadian, Jasreet Hundal, Allegra A. Petti,
Amy Ly,
Wen-Rong Lie, William H.
Hildebrand, Elaine R. Mardis,
Gerald P. Linette A dendritic cell vaccine increases the
breadth and diversity of melanoma neoantigen-specific T cells, Science DOI: 10.1126/science.aaa3828
Getting Personalised with
Neoantigen-based therapeutic Cancer, Cancer Immunol Res; 1(1); 11–15. ©2013 AACR.
Richard Aplenc, David M. Barrett, Nancy J. Bunin, Anne Chew, Vanessa E.
Gonzalez, Zhaohui Zheng, Simon F. Lacey, Yolanda D. Mahnke, Jan J. Melenhorst,
Susan R. Rheingold, Angela Shen, David T. Teachey, Bruce L. Levine, Carl H.
June, David L. Porter, Stephan A. Grupp, Chimeric Antigen Receptor T Cells
for Sustained Remissions in Leukemia, New England Journal of Medicine 2014; 371:1507-1517
Alderton, Tumour Microenvironment Driving Relapse Nature Reviews Cancer 15, 195 (2015)
of colorectal cancer Nature
Reviews Clinical Oncology March 17 2015
of tumour micro-environment heterogeneity on therapeutic response Nature
2013 501, 346–354
Cheng, Guoguang Zheng The impact
of tumor microenvironments on stem cells, Translational Cancer Research, Vol 2, No 5 (October 2013)
fronts in an old war, Nature 2006 442.7104:735-735
The root of the problem, Nature 2006 442.7104: 742-3.
Woodcock, Martha Brumfield,
Dalvir Gill, Elias Zerhouni, The driving role of consortia on the
critical path to innovative therapies Nature Reviews Drug Discovery 13, 781, 2014
Biomarkers in Risk Assessment: Validity and Validation. Accessed: April 8 2015, Accessible from: http://www.inchem.org/documents/ehc/ehc/ehc222.htm.
Wang, Emily H Cheng, James J Hsieh, Taspase1
cleaves MLL1 to activate cyclin E for HER2/neu breast tumorigenesis, Cell Research 2014 Nov; 24(11): 1354–1366.
Alvarez, Christopher G. Duncan, Ryo Nishikawa, Motoo Nagane, An-Jey A. Su,
Philip E. Auron, Matthew L. Hedberg, Lin Wang, Jeffery J. Raizer, John A.
Kessler, Andrew T. Parsa, Wei-Qiang Gao, Sung-Hak Kim, Mutsuko Minata, Ichiro
Nakano, Jennifer R. Grandis, Roger E. McLendon, Darell D. Bigner, Hui-Kuan Lin,
Frank B. Furnari, Webster K. Cavenee, Bo Hu, Hai Yan, and Shi-Yuan Cheng, EGFR phosphorylation of DCBLD2 recruits
TRAF6 and stimulates AKT-promoted tumorigenesis, Journal of Clinical Investigation 2014 Sep 2; 124(9): 3741–3756.
chemoresistance: tumor-associated stromal cells protect tumor cells from cell
death, International Journal of
Molecular Science. 2012;13(8):9545-71
Toshiharu Kamura, Masamichi Kojiro, Angiogenesis
in Cancer, Journal of Vascular
Health Risk Management 2006 Sep; 2(3): 213–219
NSW Clinical Trials Business Development Centre, 2008, Value of Industry Sponsored Clinical Trials in Australia: Inaugural
Survey of Investigator Perceptions of the Value of Industry Funded Clinical
Research
Derek J Ward, Orsolina I Martino, Sue Simpson, Andrew J Stevens, “Decline
in new drug launches: myth or reality? Retrospective observational study using
30 years of data from the UK“, BMJ
Open 2013;3:e002088
Solutions Blog, “NME Output versus R&D Expense – Perhaps there
is an explanation”, Accessed
May 2014, retrieved from: http://www.discoverymanagementsolutions.com/the-organization-of-biopharmaceutical-rd/common-goals-between-discovery-and-development/innovation/nme-output-versus-rd-expense-perhaps-there-is-an-explanation/#comment-698
J Cohen “Macrotrends in pharmaceutical innovation” Nature Rev.
Drug Disc. 2005, 4, p78-84
J Kaitin “Deconstructing the Drug Development Process”, Clinical Pharmacology and Therapeutics 2010
87 p356-361
Inc. Financial Report 2007, Pfizer Inc 2008, retrievable from http://www.pfizer.com/files/annualreport/2007/financial/financial2007.pdf
Inc. Financial Report 2008, Pfizer Inc 2009, retrievable
from http://www.pfizer.com/files/annualreport/2008/financial/financial2008.pdf
Inc. Financial Report 2009, Pfizer Inc 2010, retrievable
from http://www.pfizer.com/files/annualreport/2009/financial/financial2009.pdf
Inc. Financial Report 2010, Pfizer Inc 2011, retrievable
from http://www.pfizer.com/files/annualreport/2010/financial/financial2010.pdf
Inc. Financial Report 2011, Pfizer Inc 20012, retrievable
from http://www.pfizer.com/files/annualreport/2011/financial/financial2011.pdf
biologics, PharmaTimesDigital, March
21 2012, Accessed 12 April 2015, accessible from: http://www.pharmatimes.com/article/12-03-21/Pharma_patent_filings_fall_amid_shift_to_biologics.aspx
Joseph Barfett, Brett Lanting, Julian Lee, Michael lee, Victor Ng, Peter
Simkhovitch, “Pharmaceutical Marketing to medical Students; The
Student Perspective” Medical
Journal of Malaysia 2004 8: 21-27
Myoung Cha, Bassel Rifai, Pasha Sarraf, Pharmaceutical forecasting:
throwing darts? ” Nature
Reviews Drug Discovery 12, 737–738 (2013)
R&D FACTBOOK, thompson and Rheuters Report, June 2012, Accessed 10
April 2015, Accessible from http://cmr.thomsonreuters.com/pdf/2012-cmr-factbook-exc_cbr-en.pdf
[46] Aidan Hollis, 2004, “Me-too drugs: is there a problem? ” Department of Economics, University of
Calgary, Dec 2004. Accessed April 2014, Accessible from: http://www.who.int/intellectualproperty/topics/ip/Me-tooDrugs_Hollis1.pdf
Henry Grabowski and Margaret Kyle, 2007, “Generic Competition and
Market Exclusivity Periods in Pharmaceuticals” Managerial and Decision Economics 2007 27:
1–12
Omudhome Ogbru, “Why Drugs Cost So Much”, MedicineNet 2012, Accessed April 2014, Accessible from http://www.medicinenet.com/script/main/art.asp?articlekey=18892
Pedro Cuatrecasas 2006, Drug discovery in jeopardy J Clin Invest.
2006;116(11):2837–2842
Alison Evans, Clinical Oncology Society of Australia, Australian Neuroendocrine Tumours (NETs) Consensus Workshop Report
Meeting Management Challenges in Australia Summary Report, September 2008, Accessed 19 April 2015,
Accessible from: https://www.cosa.org.au/media/1060/cosa_report_nets-consensus-workshop_2008.pdf
of Health Economics 2003.
DiMasi, J. A., H. Grabowski, Health
Economics of new oncology drug development. Journal of Clinical Oncology, 2007 10, 209–216
Biotech Different?, Managerial and Decision Economics,
2007″,
]73] Sandra
Peters, Tufts Center for the Study of Drug Development, Cost to Develop and Win
Marketing Approval for a New Drug Is $2.6 Billion Press Release, November 18, 2014, Accessed April 10 2015, accessible
from: http://csdd.tufts.edu/news/complete_story/pr_tufts_csdd_2014_cost_study
Drug Development Costs“. Journal of Health Economics, 2003 Mar;22(2):151-85
Drug Administration, Innovation or Stagnation:
Challenge and Opportunity on the Critical Path to New Medical Products,
Challenges and Opportunities Report – March 2004, Accessible from: http://www.fda.gov/ScienceResearch/SpecialTopics/CriticalPathInitiative/CriticalPathOpportunitiesReports/ucm077262.htm
Drug Development Process, FDA factsheet, viewed April 2014,
retrieved from: http://patientnetwork.fda.gov/learn-how-drugs-devices-get-approved/drug-development-process
in new drug development: approval success rates for investigational drugs. Clinical Pharmacology Therapy, 2001
May;69(5):297-307.
Truly Staggering Cost of Inventing New Drugs, Forbes Business Feb 2012, Accessed March 2014, Accessible from: http://www.forbes.com/sites/matthewherper/2012/02/10/the-truly-staggering-cost-of-inventing-new-drugs/
Trade Related Aspects of Intellectual Property Rights, Including Trade in
Counterfeit Goods“ World
Trade Organisation Doha Decleration, 319-351, 1994
Andersson, F. Hertzmant, P, 1993, “Effective
Patent Life of Drugs in Sweden. A comparison with International Studies,”
Managerial and Decision Economics 1993 14
(1), 53-63
Laura Magazzini, Fabio Pammolli, Massimo Riccaboni, R&D Productivity, Spillovers and Effective Patent
Life” Nature Reviews Drug
Discovery 10, 428-438 (June 2009)
Accenture, The New Reality: Maximizing
Product Launches in the Post-Blockbuster World Report, 2012, Accessed April 18 2015, Accessible from: http://www.accenture.com/SiteCollectionDocuments/PDF/Accenture-The-New-Reality-Maximizing-Product-Launches-in-the-Post-blockbuster-World.pdf
Goldacre, Ben. Bad Pharma; How Drug Companies
Mislead Doctors and Harm Patients. Print. Faber & Faber;
Reprint edition (February 5, 2013
Australian Government Department of Industry And Science, Review of the
literature on participation in clinical trials: barriers and incentives for
health care practitioners and consumers, Australian clinical Trial Website, Accessed 17 April 2015, Accessible
from: http://www.industry.gov.au/industry/IndustrySectors/PharmaceuticalsandHealthTechnologies/National-Survey-and-Literature-Review/Documents/BiotextReport.pdf
August 8 2014, Transcript available on request
Stead D Cameron, Lester, M Parmar, R Haward, R Kaplan, T Maughan, R Wilson, H
Campbell, R Hamilton, D Stewart, L O’Toole, D Kerr, V Potts, R Moser,J
Darbyshire, P Selby, Strengthening
clinical cancer research in the United Kingdom British Journal of Cancer. 2011 May 10; 104(10): 1529–1534
EUROCARE-2 Study. International Agency for Research on Cancer
Publications 1999 No. 151. Originally
published Ann Ist Super Sanità
2009 Vol. 45, No. 3: 315-324
Working Group. 1999. Strategic priorities in cancer research and development. Department of Health: England
Cameron, M. Stead, N. Lester, M. Parmar, R. Haward, T. Maughan, R. Wilson,A.
Spaull, H. Campbell, R. Hamilton, D. Stewart, L. O’Toole, D. Kerr, V. Potts,R.
Moser, M. Cooper, K. Poole, J. Darbyshire, R. Kaplan, M. Seymour, P. Selby, Research-Intensive Cancer care in the NHS
in the UK, Annals of Oncology, Vol
22, issue 7, pvii 29 – pvii 37
Rachet B, Maringe C, Nur U, Quaresma M, Shah A, Woods LM, Ellis L, Walters S,
Forman D, Steward J, Coleman MP. Population-based
cancer survival trends in England and Wales up to 2007: an assessment of the
NHS cancer plan for England. Lancet
Oncology 2009 Apr;10(4):351-69.
Bois A, Rochon J, Lamparter C, Pfisterer J; AGO Organkommission OVAR
PFisterer., Pattern of care and impact
of participation in clinical studies on the outcome in ovarian cancer, Lancet International Journal of
Gynaecological Cancer. 2005 Mar-Apr;15(2):183-91.
Majumdar SR, Roe MT, Peterson ED, Chen AY, Gibler WB, Armstrong PW. Better outcomes for patients treated at
hospitals that participate in clinical trials. Archives of Internal Medicine 2008 Mar 24;168(6):657-62.
Commonwealth of Australia, 2009, Pharmaceuticals
Industry Strategy Group – Final Report Accsessed April 2014, Accessible
from: http://apo.org.au/research/pharmaceuticals-industry-strategy-group-final-report
2011
Ashworth M, et al. Cluster randomised
trial in the General Practice Research Database: 1. Electronic decision support
to reduce antibiotic prescribing in primary care (eCRT study). Trials2011;12:115.
of 49 executives and chief risk officers of pharmaceutical , biotech and
medical devices
Annamaria Muroni, Optimising Patients
Recuirtment and Retention in Clinical Trial, Queensland Government Education, 2007. Accessed April 2014, Accessible
from: http://www.health.qld.gov.au/pahospital/research/education/docs/05_04_11.pdf
Lara PN Jr1, Higdon R, Lim N, Kwan K, Tanaka M, Lau DH, Wun T, Welborn J,
Meyers FJ, Christensen S, O’Donnell R, Richman C, Scudder SA, Tuscano J,
Gandara DR, Lam KS. Prospective
evaluation of cancer clinical trial accrual patterns: identifying potential
barriers to enrollment. Journal
of Clinical Oncology 2001 Mar 15;19(6):1728-33
RS, Frisby KA, Lee JA, Mathiason MA, Meyer CM, Ostern JL, Walther SM, Schroeder
JE, Meyer LA, Umberger KE.Clinical
trial accrual among new cancer patients at a community-based cancer center. Cancer. 2006 Jan 15;106(2):426-33.
Thorir Bjornsson, May 2010 Does Pharmaceutical Predictivity Translate to
Productivity in Drug Development? If So, How?, presentation
to NGP Summit in Los Angeles in 2009, and at FDA in Silver Spring, Maryland,
and Critical Path Institute in Tucson, Arizona, in 2010, Accessed March 2014,
Accessible from: http://dl.dropbox.com/u/6886618/Pharmaceutical%20Predictivity%20May-2010.ppt.pdf
Tjeerd-Pieter van Staa, Jackie Cassell, Ben Goldacre, Martin Gulliford, Adel
Taweelunir Pirmohamed, Adel Taweel, Brendan Delaney, Liam Smeeth, 2011; Pragmatic randomised trials using routine electronic health records:
putting them to the test British
Medical Journal 2012;344:e55
2014, accessed 19 April 2015, accessible from: http://www.computerweekly.com/news/2240215074/NHS-England-admits-failure-to-explain-benefits-of-caredata
Executive Summary of a Policy Position Paper From the American College of
Physicians, Annals of
Internal Medicine 2015;162(4):301-303
Internal Medicine 2015;162(4):315-316
Peter B. Jensen,, Lars J.
Jensen1 and
Søren Brunak Mining electronic
health records: towards better research applications and clinical care, Nature Reviews Genetics, June 2012, 13:395-495
Kroger Pharmacy, Data and Text Mining the Electronic Medical Record to Improve
Care and to Lower Costs, Data Mining and Predictive Modeling, Paper 077-31,
of Novel Combination Therapies New England Journal of Medicine
2011; 364:985-987
Engelman
JA, Zejnullahu K, Mitsudomi T, et al. MET amplification leads to gefitinib resistance in lung cancer by
activating ERBB3 signaling. Science 2007;316:1039–43.
M, Faber AC, Wang SE, et al. Acquired resistance to EGFR tyrosine kinase inhibitors in cancer cells
is mediated by loss of IGF-binding proteins. J Clin Invest 2008;118:2609–19.
Zhu Shuning A. Gai Cary F. Opel12 Byron H. Kwan Rishi Surana Martin C. Mihm
Monique J. Kauke Kelly D. MoynihanAlessandro Angelini. Robert T. Williams.
Matthias T. Stephan. Jacob S. Kim. Michael B. Yaffe. Darrell J. Irvine. Louis
M. Weiner.Glenn Dranoff. K. Dane Wittrup, Synergistic
Innate and Adaptive Immune Response to Combination Immunotherapy with
Anti-Tumor Antigen Antibodies and Extended Serum Half-Life IL-2, Cancer
Cell Volume 27, Issue 4, p489–501, 13 April 2015
NK, Sproesser K, Nguyen TK, et al. The mitogen-activated protein/extracellular signal-regulated kinase
kinase inhibitor AZD6244 (ARRY-142886) induces growth arrest in melanoma cells
and tumor regression when combined with docetaxel. Clinical Cancer Research 2008;14:230–9.
D, Belvin M, Guan J, et al. Combination
of class I PI3K inhibitor, GDC-0941, with standard of care therapeutics results
in enhanced anti-tumor responses in human cancer models in vitro and in vivo. European Journal of Cancer
Supplements 2008;6:69–70.
Kekre, John Koreth, Novel strategies to
prevent relapse after allogeneic haematopoietic stem cell transplantation for
acute myeloid leukaemia and myelodysplastic syndromes, Current
Opinion in Hematology 2015, 22 (2): 116-22
Hochhaus, F Giles Novel
myelofibrosis treatment strategies: potential partners for combination
therapies Leukemia: Official Journal of the Leukemia Society of
America, Leukemia Research Fund, U.K 2014, 28 (11): 2139-47
C Pasquini
regimens for lymphoproliferative disorders Bone Marrow Transplantation 2015, 50 (3):
367-74
therapy reform. Science 2010;328:137-137
unmarketed investigational drugs for use in combination. Food and Drug Administration, December 2010
(draft). Accessed April 10 2015, Accessible from: (http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM236669.pdf.)
Consortia-Pedia, An In Depth Look at the
Research-By-Consortium Trend in Medical Research and Development, 2014
clinical trials. Semininars in Oncology
Nursing 2012 May;28(2):116-21.
Development for Rare and Neglected Diseases and Individualized Therapies:
Workshop Summary., Development, and Translation. Washington (DC): National Academies Press (US); 2009.
Accessed 15 April 2015, Accessible from: http://www.ncbi.nlm.nih.gov/books/NBK50977/
new drugs: Who contributes how much. In: Burke MA, ed. Monitoring the financial
flows for health research 2005: behind the global numbers. Global Forum for Health Research, 2006:27-43
Gambrill S. Venture philanthropy on the
rise. The CenterWatch
Monthly. 2007;14(8):6–14
Accessed April 10 2015, Accessible from:
http://www.curebraincancer.org.au/page/13/research-strategy
collaboration, Accessed: April 10
2015, Accessible from: http://www.curebraincancer.org.au/news/20/media-release-charlie-teo-announces-global-brain-exchange-collaboration
behavior and health education research, Health Education Research (1993) 8 (4):589-593
the Cancer Genome, A guided tour through the
main online resources for analyzing cancer genomics data, The Scientist
Magazine, March 1, 2012, Accessed: 20 April 2015, Accessible from: http://www.the-scientist.com/?articles.view/articleNo/31747/title/Combing-the-Cancer-Genome/
Medical Calculation Apps, Journal of
Medical Internet Research 2014 Feb; 16(2): e32
Review, Victoria Department of
Health, June 2012, Accessible from: www.health.vic.gov.au/cancer
Weller D. Primary care oncology:
essential if high quality cancer care is to be achieved for all. Family Practice. 2002 Dec;19(6):577-8.
Saunders, Sandra C Thompson, Lorna K Rosenwax, Scott Sargant, Eric L Khong,
Georgia K B Halkett, Gloria Sutherland, Hooi C Ee, Tanya L Packer, Gareth
Merriman, Hayley R Arnet, Timely cancer
diagnosis and management as a chronic condition: opportunities for primary
care, Medical Journal of Australia
2008; 189 (2): 78-82.
Foreman L, Foreman L. Bowel cancer
screening–a role for general practice. Australian
Family Physician. 2009 Apr;38(4):200-3.
Barnett Nicholas Graves Funding:
Australia’s grant system wastes time, Nature
495, 314, 21 March 2013
among patients with cancer and oncologists, Community Oncology, Volume 6/Number 5, May 2009, 207-228
and personal communications, April 23 2015, e-mail interactions available on
request