So this all started from a Facebook discussion. Yet again, I found myself trying to reason with a brick wall of denial, conspiracy theories and anti-science, baseless rhetoric that is often espoused from the mouth of a “woke” hippy. Towards the end of it, as many who defend Alternative Medicine end up claiming, the lady I was talking to said, “The ONLY reason why there isn’t research for this is because BIG PHARMA can’t PROFIT from anything nAtUrAl.” And that from there, this lady went on to insinuate that 10million researchers and doctors, along with half or billion or so who work in health or health administration, were all in on a conspiracy to suppress the potential for elderberries to cure cancer.
Of course, she’d later go on to PM me her discount code, and an amazing opportunity to become part of an organisation that brings alternative therapies like those berries to the public, out of the Goodness of their hearts (it WAS only $99.99 to SIGN UP to the first pack which I could onsell to others – in other words an MLM scam). But by this stage I’d had enough.
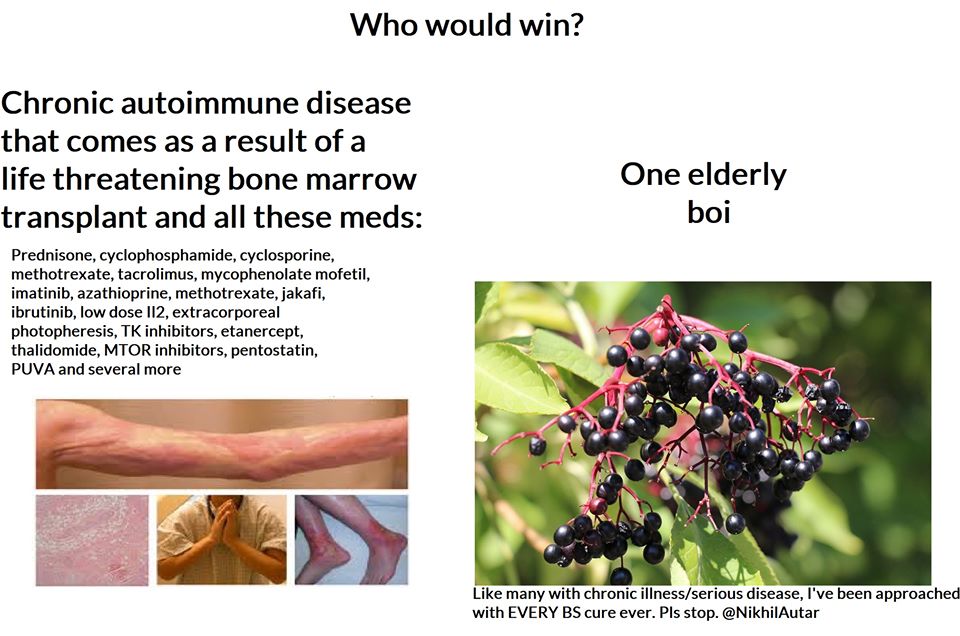
Not only did it inspire this meme… It also got me to tear down her argument piece by piece.
Because pharmaceuticals, though they are HIGHLY unethical in their practices, unscientific themselves, and RICH as HELL – are not stupid.
And in the end, despite all their evils (and yes, I DO think many are just that), they, through the research and innovation they fund, ARE the reason we’ve got SUCH amazing healthcare, and why we’ve come SO far as a society, and species over the last century.
The way the world works, to ensure we get safe, effective drugs – a process which relies on research that costs millions (sometimes tens to hundreds of millions) to execute, literally over a decade to conduct, for a marginal, 6% chance of success IF it reaches human trials – pharmaceuticals NEED to make BILLIONS to justify their existence. To get one successful drug out there to market, it costs pharmaceuticals $2.5billion in research and development, in fact.
I mean think about it – if I came up to you, and asked you to give me $10,000 today… and that it’d take me at least 10, maybe 15 years to get it back to you… and that there’s a 94% chance you wouldn’t see that $10,000 ever again, you’d wanna get at least $1 million in return right?
Well, so do investors. That’s why laws are developed to allow a company that patents a drug and invests those millions into it, can set whatever price they want to and ensure themselves a monopoly – to allow for such expensive, time consuming research to occur.
That doesn’t justify them doing the abhorent, unethical things they do to sell these products though. Pharmaceuticals spent just 16% of their budgets on research and development these days compared to 30% a few years ago. They spend sometimes over HALF on SALES. And what does sales involve? Often, the most effective strategy to sell a drug, when it’s only able to be accessed by someone who’s trained to do so is to “incentivise” or pretty much, Bribe, doctors who prescribe medicines. There is ONE SALES REPRESENTATIVE (who are generally very well paid) FOR EVERY 10 DOCTORS in the US. That’s how lucrative this industry is – doctors are RICH. If you can invest that much into sales reps and turn a profit, that says something about the influence these untrained, not-necessarily-science-literate people have on prescribing practices!
It not only leads to people not getting the medicine they should be getting, it also corrupts science. Studies funded by big pharma are 85% likely to show positive results, as opposed to government funded ones (50%) and foundation/not for profit sponsored trials (72%).
The opioid epidemic IS something that’s been made a problem by ONE big pharmaceutical. And it’s resulted in over half a million deaths and infinitely higher rates of addiction in the US – and the family that facilitated it earned MORE from its sales than it’s being forced to pay out in fines. Though they may not get away with it entirely, I’m sure they’re praising themselves for making the correct business decision in doing so, the pure evil family behind this (John Oliver breaks this down brilliantly, here).
And because this industry is much more nuanced than anything I could go into in a singular blog post – not only because it’s healthcare, and everyone and every disease is different – but also for the rules and regulations that are involved in it… I’ve decided to just focus in on one issue that consistently gets brought up here.
The conspiracy theory espoused by many that Big Pharma is hiding the cure for it all. That this logistically could be done.
That companies or individuals would forgo opportunities to make billions of dollars to do so just to stick it to the common man (including their own family members)
And that pharmaceuticals are not able to, or not currently profiting from, therapies that come from natural alternative sources.
And in doing so, I’ll turn it back around. If it IS indeed possible to profit from supposed “miracle cures” that so many people swear by, is it more likely that there’s a huge conspiracy to suppress something that “freedom fighting,” “woke,” alternative practitioners and internet researchers are trying to dispel, or is it more likely that a $210billion, unregulated, complimentary/wellness/organic industry has a lot more to gain by spreading this kind of doubt, and profiting the easy way – by investing everything in fancy marketing and absolutely ZERO in actual research.
This is the actual trailor of “formidable mind” (formidable only because it’s one that’s never been used before) Gwyneth Paltrow’s new educational documentaries (obviously ranked less the lowest rung on the ladder that is the heirachy of clinical evidence), “Goop Lab.” I swear to God, the last 40 seconds is not edited in any way. That’s literally what they shot as a trailer. WTF?
So without further ado, here’s how I took on this hun trying to convince me, someone who’s written papers on the evils of the pharmaceutical industry (and who’s never been paid by them or given anything free by them) and how we can improve its efficiency, that there’s a HUGE conspiracy to HIDE THE CURE for EVERYTHING by, apparently, EVERYONE.
(She’d just linked me a documentary of I-can’t-remember-exactly-what to back up her assertions to contextualise things. This is something you may reguarly see from an irate me in the comments section of my Faeebook page – check that out if you have the time).
“Movies, memes and documentaries are not evidence. Hell, even what a doctor says is not evidence. It’s the lowest level of evidence and not recommended for use at all. Why? Because anyone can say anything. The benefit of science and evidence is that ANYONE can test and reproduce your findings to validate if what you’re doing is right. Individual practitioner experience is helpful in making decisions, yes, but we don’t use it for a reason. It’s what we did 1 – 2 centuries ago exclusively, back when our life expectancy was 40.
Without evidence, and indeed, big pharma, we wouldn’t have the drugs, quality of life, and life expectancy we have today – nearly 80 in most developed countries.
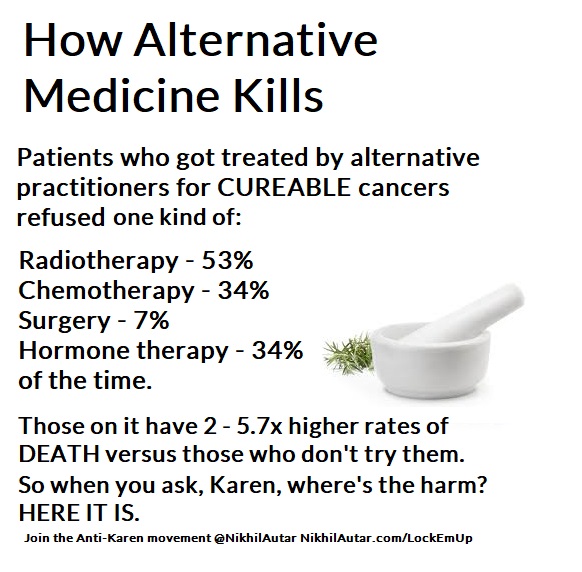
There are numerous, independent studies done on alternative medicines which show higher rates of death in patients who take them. These are patients who take them and avoid chemo and those who take them with chemo. It’s been shown that people who use alternative medicines are more likely to avoid sane, logical options for things that are shown to improve life expectancy, due to people like you, who spread misinformation. Some alternative medicines interact with and reduce efficacy of chemos (eg high antioxidant diets stop the effect of some chemotherapy regimes which use oxidation as a primary mechanism to kill cancer cells).
Why do some survive on alternative medicines though? Well,
a) There’s a chance it could be the alternative medicine. Indeed, we should study them too.
b) In many solid tumors, though, there’s a small to sometimes decent (depending on cancer, grade, lymph node infiltration, surgical outcomes etc) chance that surgery alone can cure it. Adjuvant chemo increases the odds of that immensely. Radiation post or pre chemo can too (similarly, some chemotherapies are given prior to surgery to reduce tumor volume to make surgeries more successful). So in some cases, some people do survive without chemo because of that. Likely, the ‘alternative medicine’ didn’t do anything there.
c) Some tumors also spontaneously remit – there’s a famous ‘wellness blogger’ who claimed her cancer was cured by wellness but who actually had a cancer which had a high chance of spontaneous remission is disgraced, and I believe, now sued because of this.
I talk about this, and how alternative therapies kill not only many who use them, but how they nearly killed me here – nikhilautar.com/lockemup
Is big pharma suppressing the cure? Well, you and many people don’t seem to know how the industry works, and how research works. Yes, there is investigation done into many drugs and natural remedies – a lot of blue sky research is done by universities, funded by government or by NFPs or collaborations between these bodies. But:
1) Big pharma, if they saw something had a relationship or correlation to success in alternative medicines, routinely will go out there and find a way to patent it and make BILLIONS from it anyways – even if it is ‘natural’. Contrary to popular opinion they can, and will make money off even “natural therapies” because their research and formulation is what the evidence shows and is approved by bodies like the FDA (and thus, the only legally available option of that kind for doctors to use to treat people).
Numerous drugs were traditional/natural/alternative medicines which have gone on to become multi billion dollar drugs. Paclitaxel (one of the most commonly used chemos), aspirin, various formulations of arsenic (used in some leukaemias) are famous examples of natural molecules they patented the manufacturing process of or slightly changed the molecule of, patented, and sold via sophisticated pharmaceuticals sales channels. Another example where they didn’t even change the original natural substance at all is marijuana. There’s a product which is called Sativex. It’s literally just marijuana’s main active ingredients in a specific formulation and given as a mouth spray that is now making tens of millions and will maybe make hundreds of millions/year but is no different to MJ. It’s just standardized and in a dosage and formulation they’ve studied and patented. Sativex is something my doctor wanted to use in me. So if it worked… big pharma could have and probably would have made money off it.
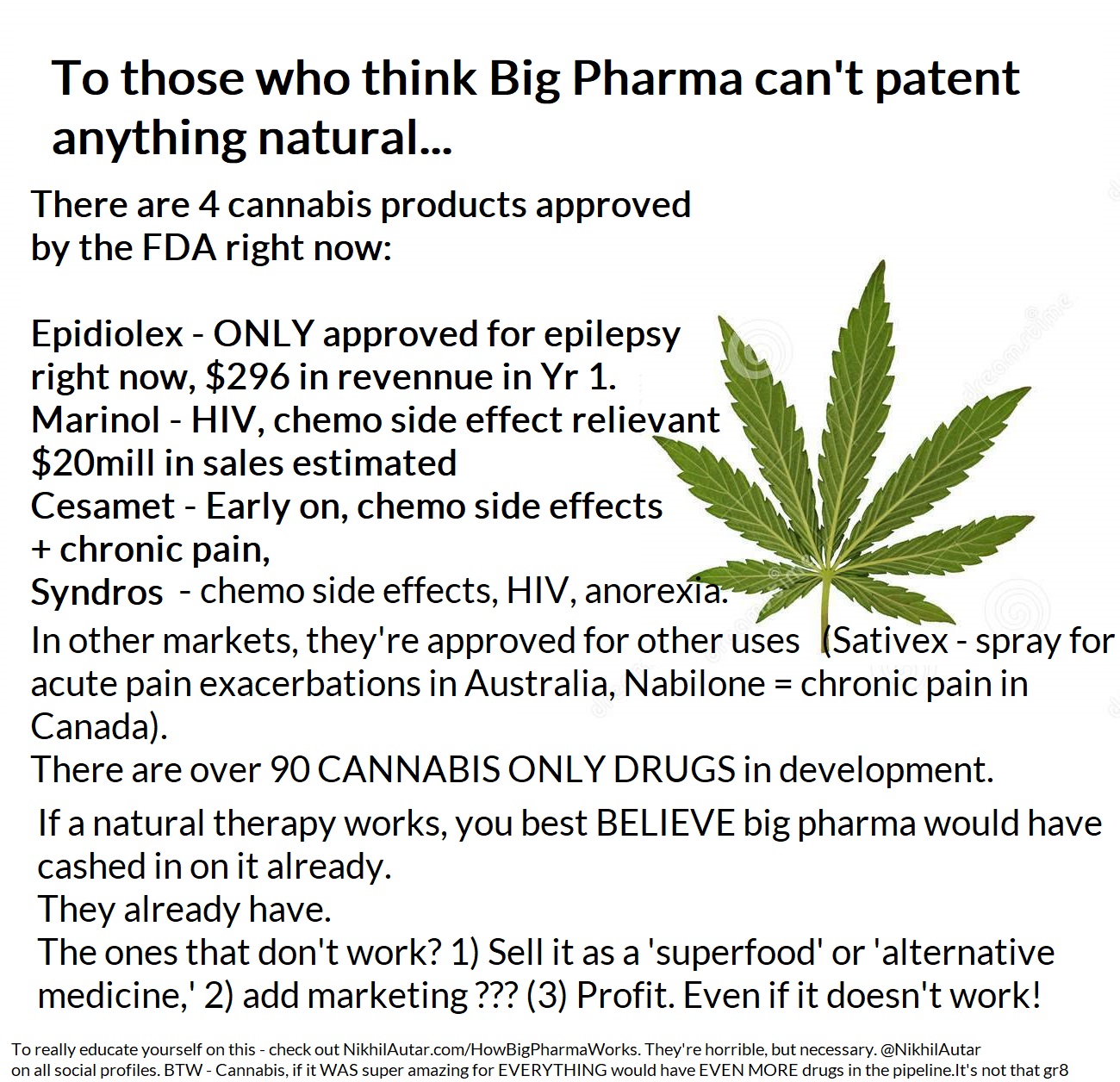
Sativex isn’t even approved in the US, I don’t think. If it was, it could have made hundreds of millions more. It’s currently going through phase 3 trials for various indications like multiple sclerosis, which may gain it approval for the US market.Weed is HIGHLY lucrative and being investigated thoroughly, though legal issues make it hard to study.
2) There are thousands – tens of thousands of companies at any one second developing drugs for various purposes as we speak. “Big pharma” isn’t just the big 5 – 10 companies which produce a fraction of the drugs that go through the pipeline. It’s a very competitive space. And though, yes, some of the big players are extremely huge, if there was something extremely promising out there, the tens – hundreds of thousands of small – large investors/venture capitalists/bankers out there who invest and often specialize in investments like this, would have jumped on it and made billions. Big pharma companies often just acquire these companies once they’ve done the hard yards, and use their extensive sales channels to distribute drugs that someone else has done the hard work/taken the huge risk in developing (only 6% of drugs that start phase 1 studies – the first stage of human trials – go on to be approved, in a 10 – 15 year process that costs millions to do, remember?). This isn’t always the case. Big pharma only invests 17% of their budgets into R&D. The rest goes into sales and M&As etc. Their tactics are highly unethical and I do hate big pharma with a passion for that reason too.
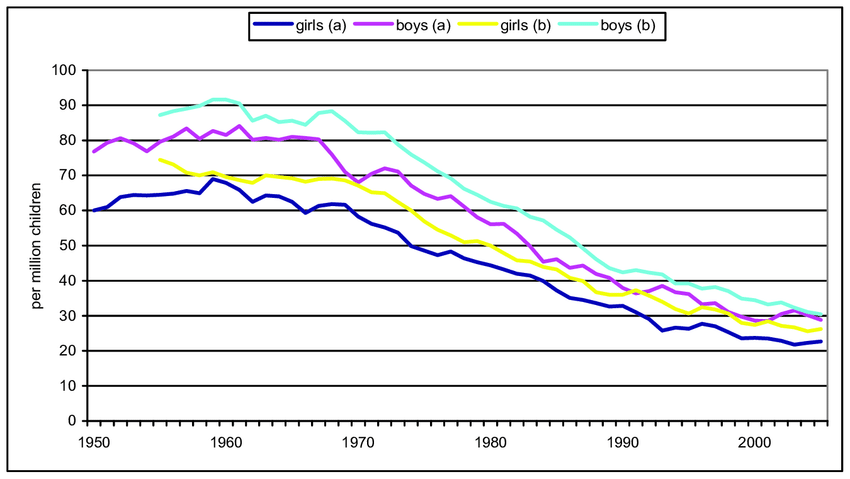
But without these big companies, we don’t get nearly as much funding for drugs, and we go wouldn’t be where we are today in terms of health outcomes. As recently as the 1990s, childhood mortality due to cancer used to be 85%. We’ve now flipped that, and childhood survival now sits at 85% in just 2 decades because of funded research.
3) There is already a LOT of research being done on various traditional/natural compounds on their ability to affect cancer. It’s not too hard or too expensive to do laboratory studies, which will be published in a journal somewhere if successful, and I know many studies are being funded through these pathways. Indeed, I have a few friends who’ve spent a year or two studying one or two in particular. My company will soon be automating medical research on consumers, and hopefully powering evidence based practice (sign up to help make this happen and win free stuff here) These (a) often haven’t been successful, or showed no results. As I said before, if they were so remarkable, big pharma would’ve pounced on them already, and (b) there’s a big problem in and of itself in that negative results often aren’t published, leading to people still insisting that things work, despite them being studied and showing limited to no success outside of early human, or petri dish studies. Petri dish, AKA laboratory studies, often don’t translate to clinical success.
Remember that 6% number? There’s many reasons for that – even a gun can kill cancer cells in a petri dish, you need to get the substance to the tumor cell, figure out how to administer it into a human body, make sure its safe and 1000 other little things to translate it into a successful drug.
It’s not as simple as “Hurr, durr, big pharma wouldn’t allow it” and “Big pharma is corrupt.”
The industry is VERY complex, but without it, we wouldn’t be where we are. Without medicines, we wouldn’t be here.
I talk about this more here. This is an essay I wrote looking into how we can continue to fund medical research in Australia which was shortlisted in an international essay competition (I believe it came in the top 5).
And yes – there is a chance a company will bury a drug that may hurt their sales overall etc. But remember also, there are thousands of companies around the world working on these problems, not just the top 10 which make up less than 1/3rd of revenues. That doesn’t mean they do 1/3rd of the research. The majority of early stage research is done by startups or small companies which will make loss for (you can’t make a penny until you have your drug approved) a decade until they get bought out by the bigger players, or raise a large amount to complete clinical trialing/start marketing etc their business.
So think more deeply before making rampant claims dudes. Because you don’t know who you’re hurting when you talk about something you know nothing about.
What are my credentials in this space? Well, not only am I a medical researcher who’s worked on a few clinical trial projects, and who’s written papers like that essay above on this topic, but I’m also the founder of a social enterprise which powers and may well automate medical research into this space.
Not only are we creating devices (something you may have heard me talk about on my various channels) that make life safer and easier for millions – something we’ve won innovation prizes and Australian Student Startup of the Year for in the past – we’re also connecting this to an AI powered app which I think has the most potential to create change.
Centered Around You, our app, will not only provide you with the most evidence based advice out there in the currently crowded, understudied (clinically at least) wellness space – in things like diet, exercise and sleep to start – but will also, through its inherent randomisation processes – collect large amounts of anonymised data that can prove if various interventions do measure up, and do what people expect they will.
Our devices, including our app, is something we’re developing to be medical devices that comply by various jurisdictions’ standards. They’re currently still under development, and in terms of the app and our first sensor devices, are currently being trialed in small user p9pulations – but we’ll need many more people to jump on board and make this a reality quicker for sure! Sign up to become a beta tester or to support at the bottom of the page on CAroundYou.com!
And do sign up for my email list to be updated of new posts on my blog too!
If you’re on YouTube – be sure to subscribe to me on that there. YouTube.com/NikhilAutar
How to Ensure Cancer Treatments Keep Imrpoving and Make the Drug Development Cycle more Efficient.