So NSW’s been swamped by COVID. We’ve got over 1200 cases per day, with cases still rising. Our vaccination rate is increasing, but the Delta virus spreads, and overwhelms hospital, even in the most vaccinated nations in the world. For some reason, in this time, our premiere wants to give up and let COVID take its course. They’re even suggesting that we stop testing. We know it’s gonna swamp our hospitals, and lead to deaths, and maybe mean we can never get this under control. It’s not just seen in other nations – it’s happening in Sydney, right now!
As usual with all my posts – all sources are linked here. I don’t have enough time to reference them all – but all science claims are backed up by relevant peer reviewed sources.

But what if I told you there’s a country that’s beaten covid back, many times, even before the vaccine, consistently without lockdowns. They didn’t even close borders. And they’re doing this with the delta strain too.
Well there is. What country is that? Iceland.
So how is Iceland, the country antivaxers said was proof vaccinations don’t work, beating COVID/doing this?
Watch this video to find out how, or keep on reading.
By testing everyone. Even asymptomatic people.
And then getting people to isolate, not just people and their households, but close contacts too for a full 14 days, and following up on them. Regularly.
Why does this work? Well, the thing that’s made COVID dangerous is the fact that you can spread it for a long time while asymptomatic. The delta strain is worse. This Nature lay person summary breaks down why well. You start detecting it at 4 days, versus 6 for other strains, and you have 1200 more viral particles than other strains too, meaning you’re more infectious, and more likely to spread it, for longer.
This probably makes testing asymptomatic people even more important.
Yet our health minister wants to stop people from getting tested. Probably because the time to getting test results back is getting too high (which is reasonable).
So how can we do what Iceland did, despite having a much larger population?
By doing something no-one else is, yet. Rapid antigen testing.
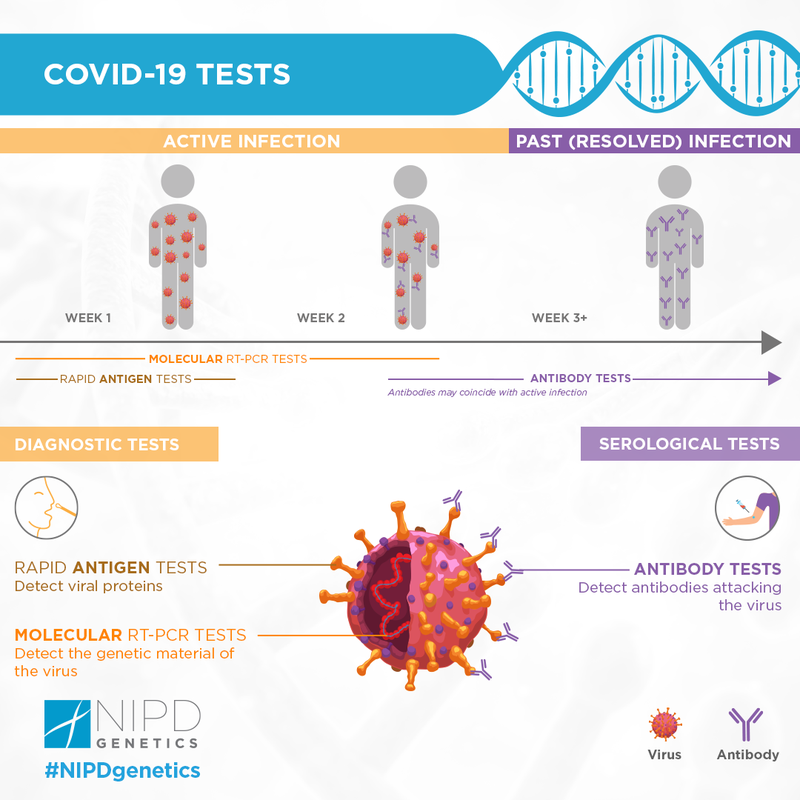
Rapid antigen tests aren’t as sensitive, but they’re cheap, can be used to test more people, more regularly, and perhaps our best way out!
PCR testing measured by labs is resource intensive. And it costs a lot too. Sydney spent over half a billion on PCR tests in the first month of the pandemic. It’s been a month since and testing has gone up MORE.
Labs earn between 60 and 120 dollars per test.
A rapid antigen test costs $5-10. Even though NSW requires healthcare staff do this, currently, other nations sell these over the counter. You could mail these out.
Yes, they’re less sensitive meaning you’ll miss more cases.
But you’ll be able to test 10, 20, maybe 30x more people at the same cost. Statistically speaking, you’re definitely, 100% gonna pick up more cases.
We do need highly accurate PCR tests for sure. But save these for people who had huge exposure, their household members and people who work in hospitals.
Give out everyone who needs to work, people in high risk areas, and more these tests, and then have them confirm this with a PCR, and we’re half way there.
This is VITAL. Not only has this been shown to work in Iceland, in real time (it’s even working against the Delta strain), we know that asymptomatic people comprise a large proportion of the actual COVID population.
The next – follow up with them REGULARLY. Call people up. Make sure they’re at home, and get close contacts to stay home and remind them to stay home too. Yes, that’s a lot of effort. But first off – we KNOW this works. Not just from Iceland. Early on in the pandemic, Italy tested 3300 people, found out 43% of cases were asymptomatic, and got these people, in addition to the symptomatic population to stay home. This is what stopped COVID-19 in its tracks.
Right now, it seems hard to do this in Sydney, a population of 6million people – 10x more than Iceland. But we have what, 21000 active cases? If you dedicated 200 of our troops (recently 500 soldiers were recruited to help this) to this for everyone, every 3 or 4 days, that’s only 10 calls a day. I did that every hour when calling people for my startup! Target inspections and house calls to those not picking up, you’ll also save money and resources doing this too!
NSW Health doesn’t release or capture data on how long people were asympomatic before becoming positive [you can estimate that info by looking at where random cases may have picked it up], this may be why we’re seeing so many people active in the community.
It’s not 100% their fault. They just didn’t know they were infected!
Almost 4 weeks ago, they were talking about rapid antigen tests. They’re already approved. I know it’s a lot of logistical work. But if someone got this out to people, we could still slow this down, rather than risk COVID spreading out of control.
If you’ve reached this point, share this with people. The more people who know about this the better. Unfortunately, noone listens to me haha. But share the video too and hopefully we can get this out there.
I’m not a public health expert, I have some relevant qualifications though. But I’m not saying we should rely on rapid antigen tests either. We need regular old, highly reliable PCR tests too. The key to Iceland’s success is they also follow up on people.
The only restrictions they’ve imposed happened very recently – to outside travellers. This strategy worked so well for them, they literally had open borders and beat back COVID every time!
I dunno about you – but I wanna fish sooner. I wanna go back to med school, knowing I’m a little bit more safe, I’m sure you wanna work too. This is a hypothesis, but something we should consider at least! Comment your thoughts below. And subscribe to my email lists to get updates on this and to keep learning.