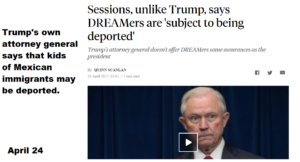
You may have heard NSW Doctors are striking right now.
As someone who’s both a doctor, on a chair, and also someone who’s had leukaemia, bone marrow transplants, open heart surgery, and so much more – someone who has to go to hospital a lot… Making sure the people who keep us safe are healthy and happy themselves is very important to me.
But I know what you’re thinking… Why are these rich aas doctors asking for a pay rise?
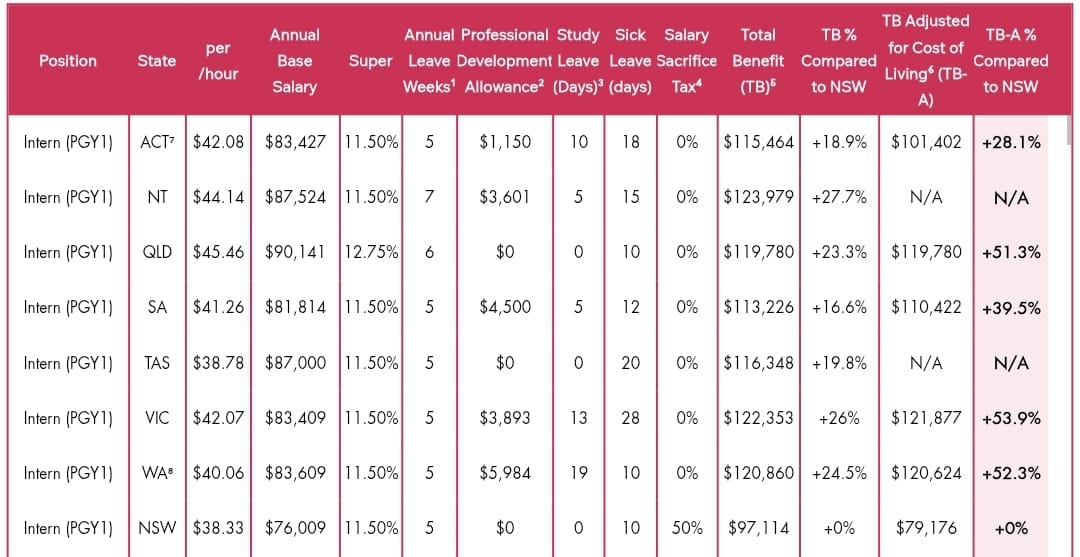
Well first off, they’re not all rich. As junior doctors, we make $38 an hour. That is more than many, but consider that this is after studying 5-10 years where we earned nothing, that we gave up our 20s, or 30s, and that we work 50-80 hour weeks while being bullied into not claiming overtime. It doesn’t go much higher than that for a while during speciality training – which is when most of us are getting married, starting families and buying houses.
Source: ASMOF
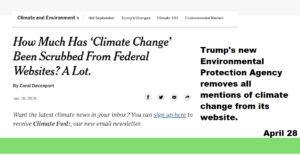
Second – because we’re getting paid 30% less than other states, doctors are leaving NSW. . And it’s not theoretical. I personally know several classmates who went to Queensland and Victoria despite wanting to stay here because the pay, staffing, hours and safety are better there. More doctors are spending more time in private practice as practicing in the public, where you earn less, and are treated worse and worse, doesn’t make sense.
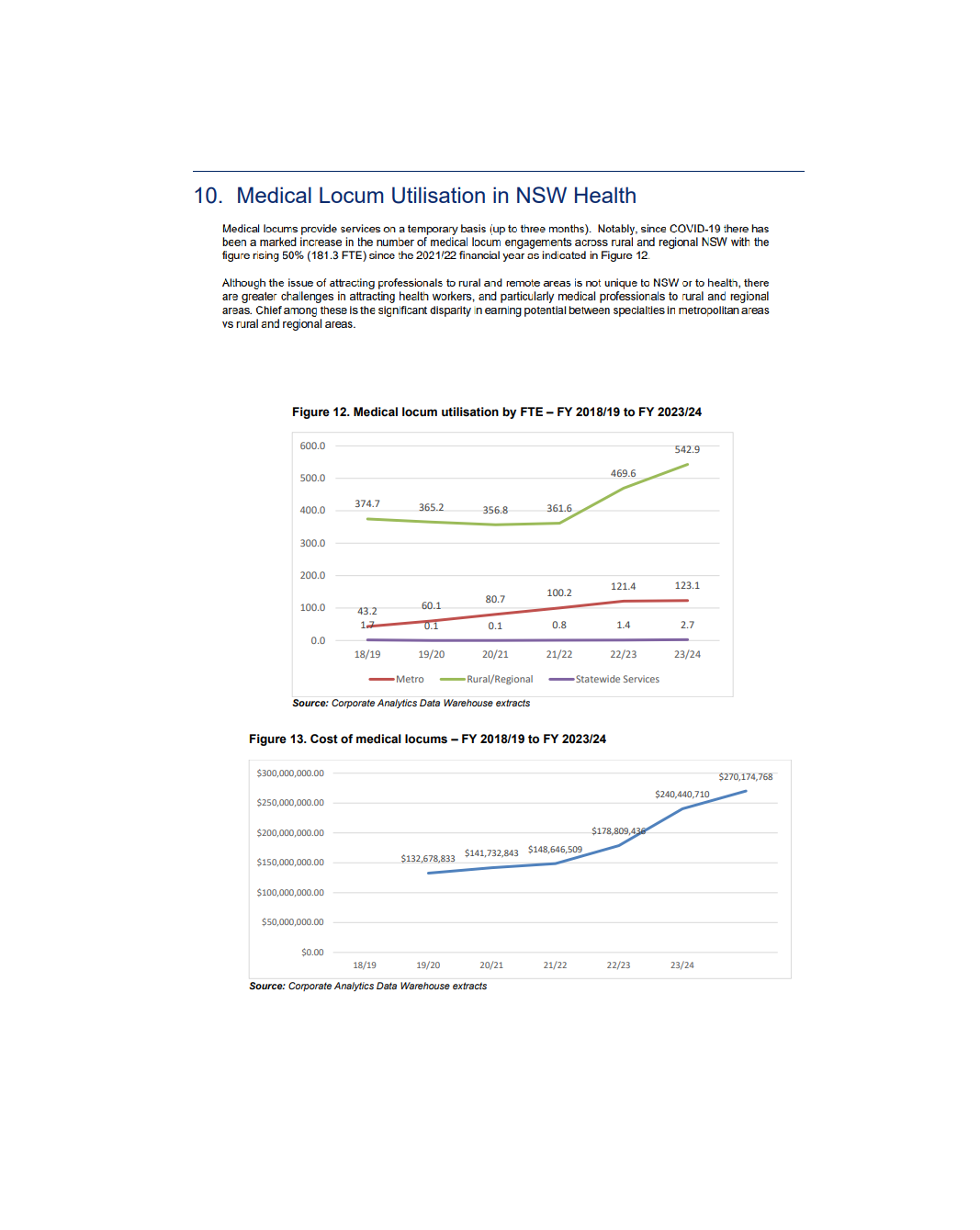
And it’s not theoretical. I personally know several classmates who went to Queensland and Victoria despite wanting to stay here because the pay, staffing, hours and safety are better there. More doctors are spending more time in private practice as practicing in the public, where you earn less, and are treated worse and worse, doesn’t make sense. There are over 900 trainee positions vacant in NSW. 29% of trainee psychiatry positions are vacant. And trainees do a LOT of the day-to-day work in hospitals.
We have the lowest rate of doctors to patients in the country – 2285 FTE per 100,000 vs 2874 in the Northern Territory, meaning doctors here have to work more, and see more patients in the same time, meaning they’re tireder and more likely to miss things when they’re treating us.
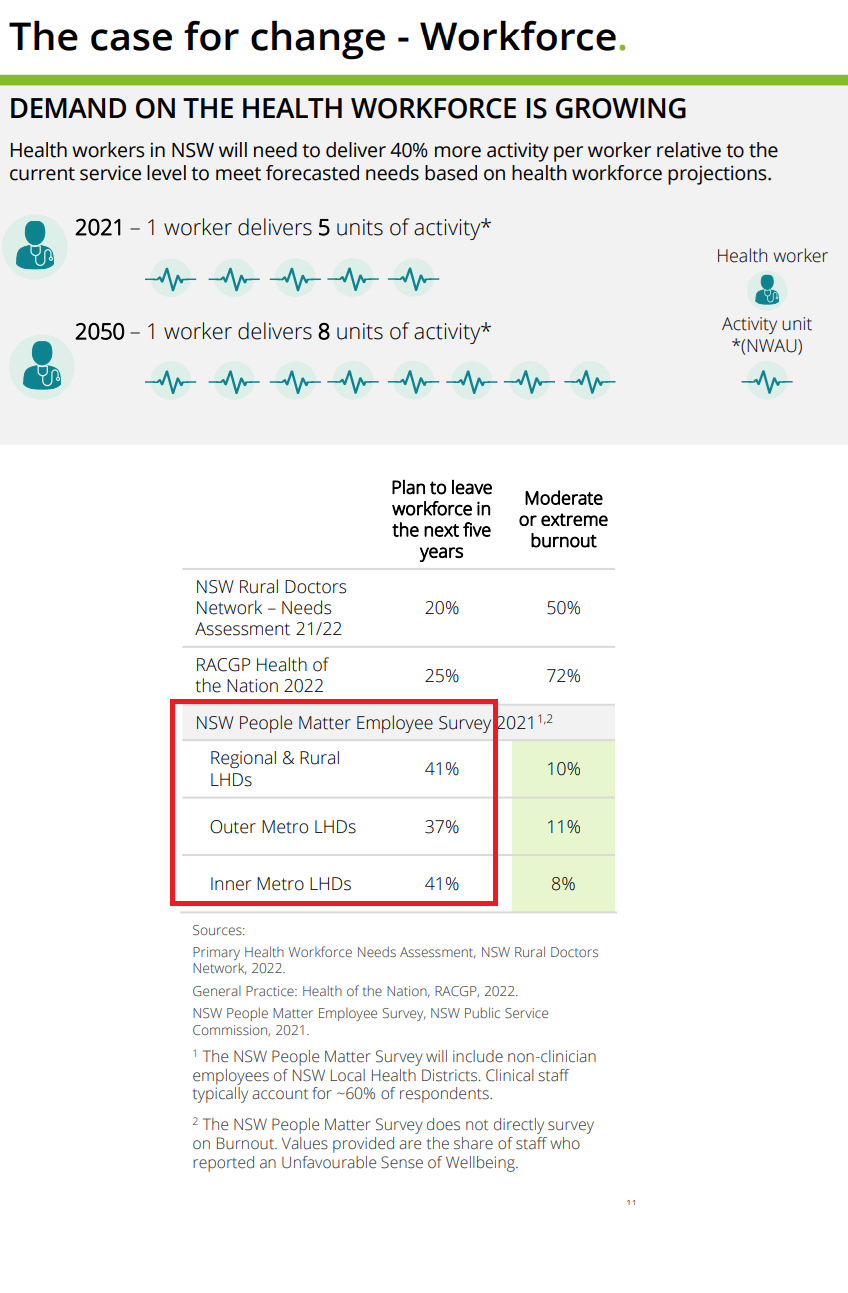
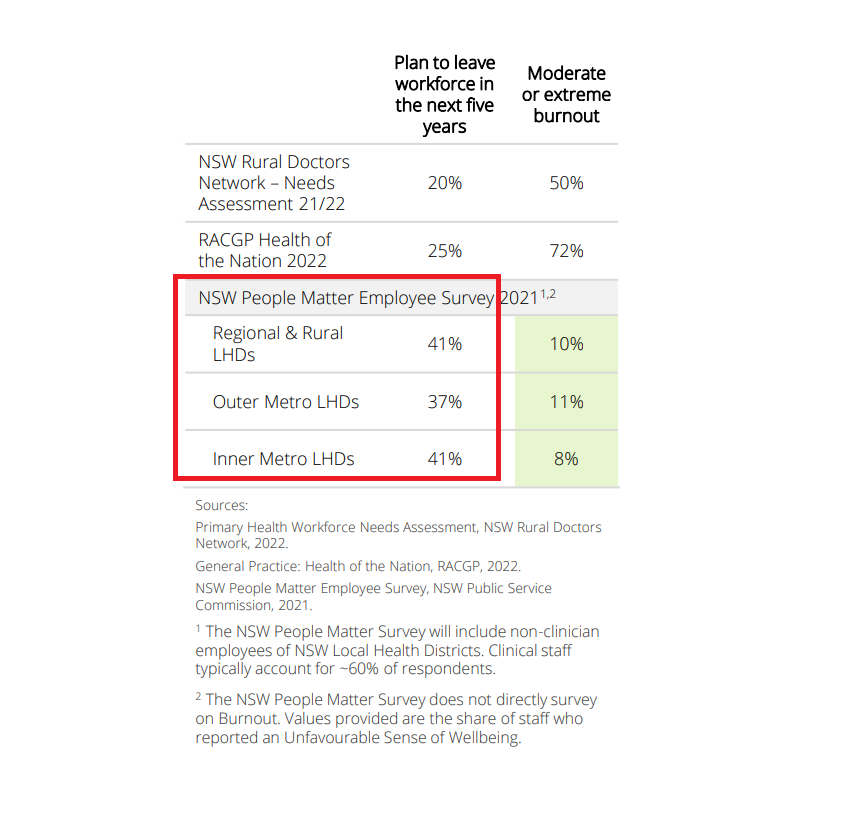
And finally, our doctors have been struggling. They had wages frozen, not getting JobKeeper, while putting their lives on the line during COVID – it’s the right thing to do. This has led to a 5% increase in attrition of the entire healthcare workforce – not just doctors. 40% of doctors plan to leave in the next 5 years, which is SCARY.
No Caption
Backing doctors, is backing all of us. So please, bring this up to your politicians, comment on social media, and talk about this, and other actions our nursing, and other colleagues are campaigning for too. It means a lot when you do!
COVID has trampled the world. My nation, Australia, is about to open up everything in the upcoming months. We’ve seen a surge in vaccination rate after an outbreak occurred in June/July – going from 11% vaccinated to 63% receiving their first dose by October 1. In the first affected state, NSW, this number is over 87% – and vaccine hesitancy is at an all time low of 8% too! A combination of messaging focusing on increasing vaccination, and restrictions promised to affect vaccinated people are to thank for this, I believe. But we’re only going for 80% vaccination. And states are starting to suggest that the unvaccinated people can enjoy these freedoms too, which may reduce vaccination enthusiasm. Here, I show real life examples from around the world which show why we need to go for 90% vaccinated to ensure Australians, including at risk people like myself, don’t suffer.
Around the world, there is reason to hope. Here are some examples of nations who have either controlled, or are starting to see huge regression of rates of COVID and hospitalisation.
The key is
They ALL have over 90% of their eligible population vaccinated.
They all test their populations and maintain excellent Contact Tracing, and have a population that abides by restrictions to people who test positive, or have symptoms.
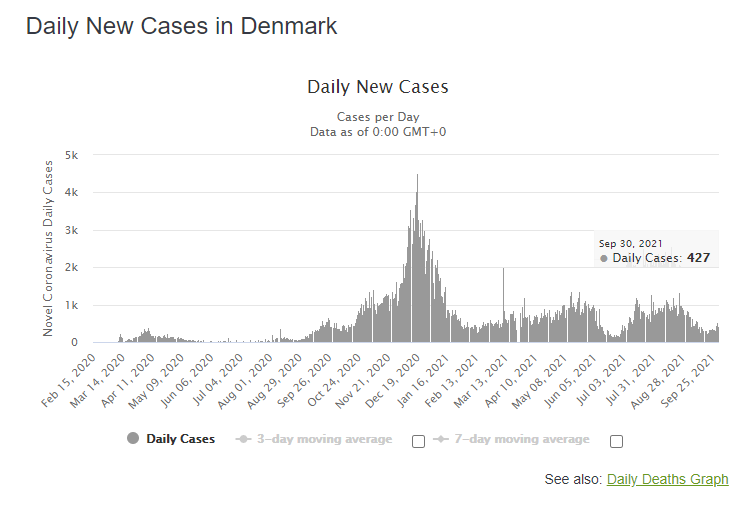
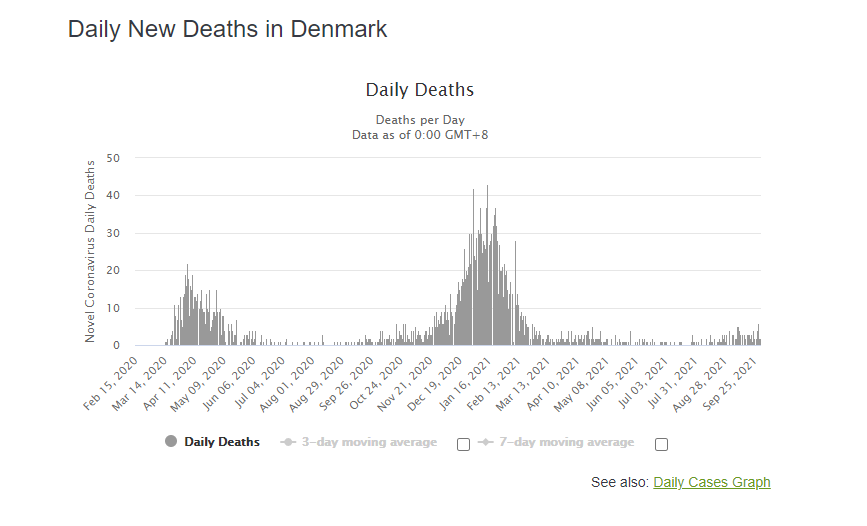
Denmark –
Just under 91% of people over 14 are vaccinated . Denmark is not seeing huge surges and has controlled their outbreak! They had a population that followed restrictions, and they mass tested (4million per week) in a national population of 6million. They only had 427 cases in a population of just under 6million yesterday (September 30, 2021). And importantly, they’ve only had 18 deaths in the last week, and no more than 6 in a day since February 2021 . In my state, we see more than that every day, recording a record 15 deaths in a day recently.
The key to their success? A population that abides by recommendations, and mass testing. They do 4million tests per week. In Sydney, at our PEAK, we were only doing 1million. I outline why this strategy works and how we can emulate this and SAVE money here.
All sourced from https://www.worldometers.info/coronavirus/country/denmark/
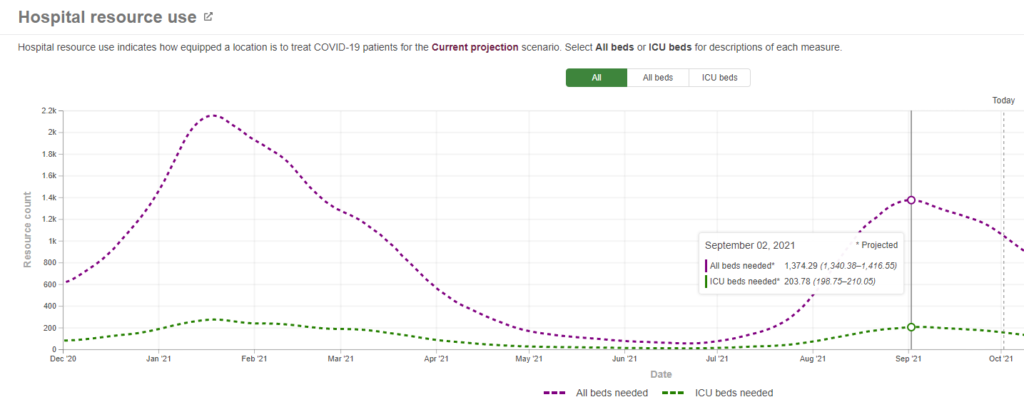
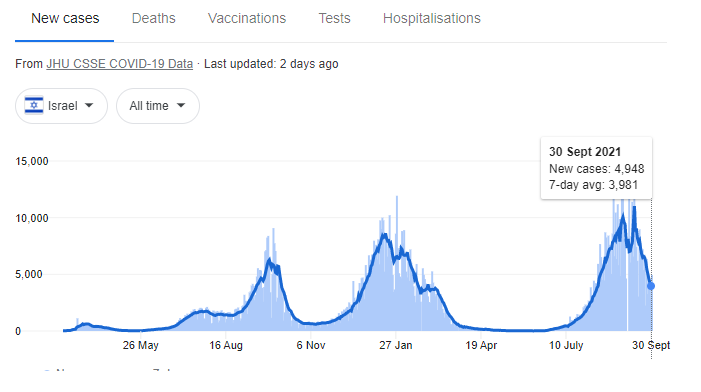
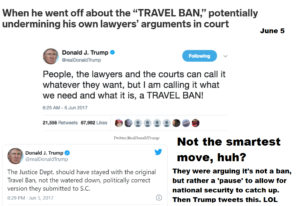
Israel
Israel has recently been maligned, and used by antivaxers as a case study of why not to vaccinate for the past few weeks. They saw 12,000 cases per day in a population of 9million – numbers similar to the US. Yet even in that time, their hospitalisation and the number of ICU beds used by COVID-19 patients were lower than the US.
Indeed, despite having over 12,000 cases per day in this recent August to September peak, they only ever needed 203 ICU beds. In my state (NSW), at 61% double-vaccinated, and less than 10% of cases, we needed more ICU beds for COVID patients – indicating how important it is we reach >90% vaccination (Israel has over 95% of its eligible population vaccinated). Sadly, 6 states had no ICU beds available in the US in late August. I personally have seen doctor friends asking hospitals interstate if they can fly patients out to get treatment via social media.
An excellent resource which also does projections. https://covid19.healthdata.org/israel?view=resource-use&tab=trend&resource=all_resources
Portugal – Reached 100% vaccination in at risk groups, and most of the nation. They too have only had 6 deaths a day as a maximum for months, are using 270 hospital beds, and need 13 ICU beds today despite seeing over 800 cases diagnosed every day! There are suggestions that hospitalisations could get worse with winter though. This is another reason why we shouldn’t be complacent and continue to contact trace and isolate those at risk, and consider restrictions to close contacts too. These aren’t lockdowns, just common sense quarantine practices! All these nations are continuing to do so.
What excites me about Portugal – they have less than 15 ICU beds dedicated to COVID-19 patients in a population of 10million!
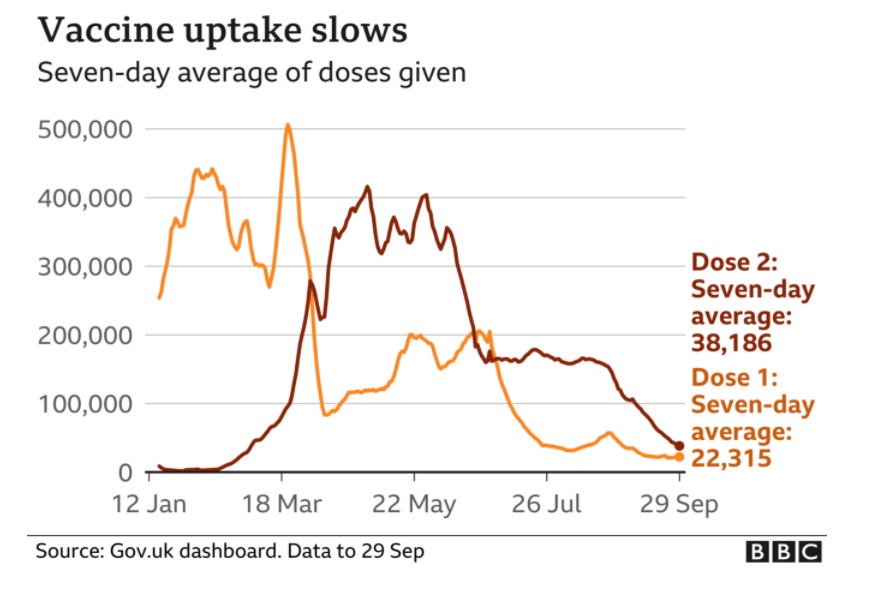
The UK
The UK has had 82% of its population double vaccinated. Yet vaccination uptake has stagnated. Unfortunately, a lot of misinformation spreads there, similar to the US. Currently, they are 130-135 deaths per day. By comparison, that would be equivalent to Australia seeing 48 deaths per day, which is almost 5x higher than what we’re seeing on average here. It’s important to know that they have almost 15x more cases per day there. So a higher vaccination rate DOES work in reducing hospitalisations. But sadly, their hospitals are quite strained – with over double the ICU bed usage (adjusted for the UK’s larger population). They did also use a different vaccine – but one shown to have similar efficacy in reducing hospitalisation and severe death against the delta strain (in any case, we in Australia also used the AstraZeneca vaccine). This is why we need a HIGHER vaccination rate than 82%!
There is reason for alarm. And this is likely why cases, deaths, and hospital strain is not going down there. I have friends in healthcare there who are struggling to keep up. I hope this trend doesn’t continue.
Iceland
Iceland has controlled the delta Virus, without lockdowns, or restrictions of any kind, at any point. They did this through mass testing and effective and comprehensive contact tracing. I discuss this in detail, and how we can use rapid antigen test screening to mitigate this. At the very least though, targeted, regular rapid antigen tests, in addition to regular PCR testing for symptomatic or exposed populations may reduce the likelihood of COVID-19 outbreaks. And we NEED to emphasise this. I feel like in NSW, we’re losing focus of this as Lockdown fatigue affects us all. Find out more on Iceland’s contact tracing strategy too.
Iceland is a great example of how mass testing and contact tracing alone works! But with a vaccination rate of >95% likely responsible for reduction in transmission, a shining example of how high vaccination helps too.
So there’s reason for hope. But I really think we need to get 90% of our population vaccinated. And continue to contact trace.
I highly recommend you subscribe to my blog for more insights like this. I’m also an ex cancer patient, cancer researcher, med tech founder and regularly debunk and campaign against misinformation.
Follow me on Facebook, Instagram and Twitter too (opens in a new link). Leave comments below too!
So NSW’s been swamped by COVID. We registered over 1400 cases per day, with numbers still rising. My already stretched hospital colleagues have received emails telling them that workloads will double in the next 2 weeks. Our vaccination rate is increasing, but the Delta virus spreads, and overwhelms hospital, even in the most vaccinated nations in the world. For some reason, in this time, our premiere and prime minister wants to give up and let COVID take its course. They’re comparing living with COVID-19, to living with the flu. They’re even suggesting that we stop testing. We know it’s gonna swamp our hospitals, and lead to deaths, and maybe mean we can never get this under control. It’s not just seen in other nations – it’s happening in Sydney, right now!
As usual with all my posts – all sources are linked here. I don’t have enough time to reference them all – but all science claims are backed up by relevant peer reviewed sources.
But there is a way we can break free of this. And we NEED to give it a shot.
There’s a country that’s beaten COVID back, numerous times – even before the vaccine – and even after the Delta strain, WITHOUT LOCKING DOWN. They didn’t even close borders. And they’ve controlled a surge of the delta strain (it surged despite >80% of the adult population being vaccinated) with this strategy.
Well there is. What country is that? Iceland.
So how is Iceland, the country antivaxers said was proof vaccinations don’t work, beating COVID/doing this?
Watch this video to find out how, and keep on reading to see EXACTLY how we could do this in NSW.
By testing everyone. Even asymptomatic people.
And then getting people to isolate, not just people and their households, but close contacts too for a full 14 days, and following up on them. Regularly.
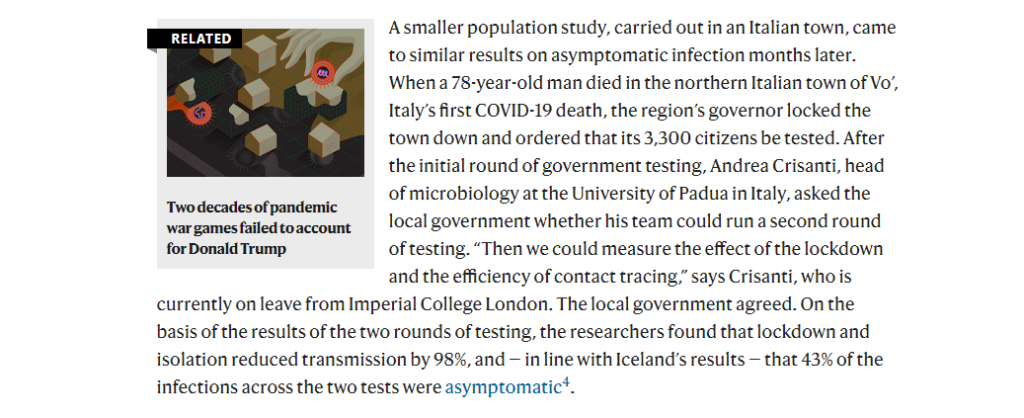
Why does this work? Well, the thing that’s made COVID dangerous is the fact that you can spread it for a long time while asymptomatic. The delta strain is worse. This Nature lay person summary breaks down why well. You start detecting the delta strain 4 days after exposure, versus 6 for other strains, and you have 1200 more viral particles than other strains too, meaning you’re more infectious, and more likely to spread it, for longer.
A lot of the time, you’ll still be asymptomatic during this. You won’t even know you’re spreading it. Which is why the delta strain’s R0 – a measure of its transmissibility – is 2 – 4x higher than previous strains.
This probably makes testing asymptomatic people even more important.
Yet our health minister wants to stop people from getting tested. Probably because the time to getting test results back is getting too high (this, at least, is reasonable).
So how can we do what Iceland did, despite having 20x more people?
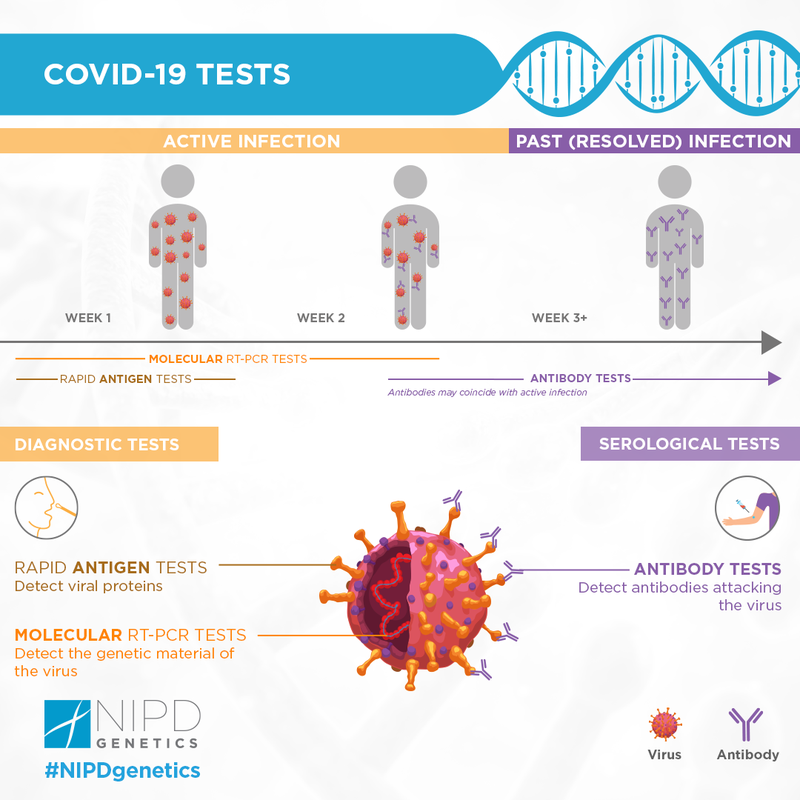
By doing something no-one else is, yet. Rapid antigen test screening.
Rapid antigen tests aren’t as sensitive, but they’re cheap, can be used to test more people, more regularly, and perhaps our best way out!
PCR testing measured by labs is resource intensive. And it costs a lot too. Sydney spent over half a billion on PCR tests in the first month of the pandemic. It’s been a month since and testing has gone up MORE.
A rapid antigen test costs $5-10. Even though NSW requires healthcare staff do this, currently, other nations sell these over the counter, and are doing them at home.
But first off – you’ll be able to test 10, 20, maybe 30x more people at the same cost. Statistically speaking, you’re DEFINITELY – 100% – gonna pick up more cases if you screen this many more poeple!
And secondly – it was found that if you repeated these tests every 3 days, the sensitivity rose to over 90% mitigating its lower accuracy.
We do need highly accurate PCR tests for sure. But save these for people who had huge exposure, their household members and people who work in hospitals.
Give out everyone who needs to work, people in high risk areas, and more these tests, and then have them confirm this with a PCR, and we’re half way there.
Right now, it seems hard to do this in Sydney, a population of 6million people – 10x more than Iceland. But we have 21000 active cases. If you dedicated 100 of our troops (recently 500 soldiers were recruited to help this) to this, calling people up every 3 or 4 days, that’s only 20 calls a day. I did that every 2 hours when calling people for my startup! Target inspections and house calls to those not picking up, you’ll also save money and resources doing this.
We spent at least $30million per day doing PCR tests.
We could do 2million screening rapid antigen tests per day, and still do over 50,000 PCR tests on those who are symptomatic, who’ve been exposed recently and for frontline workers, and SAVE money! That’s enough to screen EVERY SINGLE PERSON IN SYDNEY every 3 days!
From this, we’d
NSW Health doesn’t release or capture data on how long people were asympomatic before becoming positive [you can estimate that info by looking at where random cases may have picked it up, this may be why we’re seeing so many people active in the community.
It’s not their fault all time. Many may never have known they were infected!
I’m not a public health expert (though I have some relevant qualifications in this space and have done public health as part of my medical degree). But I’m not saying we should rely on rapid antigen tests either. We need regular old, highly reliable PCR tests too. The key to Iceland’s success is they also follow up on people.
The only restrictions they’ve imposed happened very recently – to outside travellers. This strategy worked so well for them, they literally had open borders and beat back COVID every time!
I dunno about you – but I wanna fish sooner. I wanna go back to med school, knowing I’m a little bit more safe, I’m sure you wanna work too. This is a hypothesis, but something we should consider at least! Comment your thoughts below. And subscribe to my email lists to get updates on this and to keep learning.
As usual with all my posts – all sources are linked here. I don’t have enough time to reference them all – but all science claims are backed up by relevant peer reviewed sources.
But what if I told you there’s a country that’s beaten covid back, many times, even before the vaccine, consistently without lockdowns. They didn’t even close borders. And they’re doing this with the delta strain too.
Well there is. What country is that? Iceland.
So how is Iceland, the country antivaxers said was proof vaccinations don’t work, beating COVID/doing this?
Watch this video to find out how, or keep on reading.
By testing everyone. Even asymptomatic people.
And then getting people to isolate, not just people and their households, but close contacts too for a full 14 days, and following up on them. Regularly.
Why does this work? Well, the thing that’s made COVID dangerous is the fact that you can spread it for a long time while asymptomatic. The delta strain is worse. This Nature lay person summary breaks down why well. You start detecting it at 4 days, versus 6 for other strains, and you have 1200 more viral particles than other strains too, meaning you’re more infectious, and more likely to spread it, for longer.
This probably makes testing asymptomatic people even more important.
Yet our health minister wants to stop people from getting tested. Probably because the time to getting test results back is getting too high (which is reasonable).
So how can we do what Iceland did, despite having a much larger population?
By doing something no-one else is, yet. Rapid antigen testing.
Rapid antigen tests aren’t as sensitive, but they’re cheap, can be used to test more people, more regularly, and perhaps our best way out!
PCR testing measured by labs is resource intensive. And it costs a lot too. Sydney spent over half a billion on PCR tests in the first month of the pandemic. It’s been a month since and testing has gone up MORE.
A rapid antigen test costs $5-10. Even though NSW requires healthcare staff do this, currently, other nations sell these over the counter. You could mail these out.
Yes, they’re less sensitive meaning you’ll miss more cases.
But you’ll be able to test 10, 20, maybe 30x more people at the same cost. Statistically speaking, you’re definitely, 100% gonna pick up more cases.
We do need highly accurate PCR tests for sure. But save these for people who had huge exposure, their household members and people who work in hospitals.
Give out everyone who needs to work, people in high risk areas, and more these tests, and then have them confirm this with a PCR, and we’re half way there.
Right now, it seems hard to do this in Sydney, a population of 6million people – 10x more than Iceland. But we have what, 21000 active cases? If you dedicated 200 of our troops (recently 500 soldiers were recruited to help this) to this for everyone, every 3 or 4 days, that’s only 10 calls a day. I did that every hour when calling people for my startup! Target inspections and house calls to those not picking up, you’ll also save money and resources doing this too!
NSW Health doesn’t release or capture data on how long people were asympomatic before becoming positive [you can estimate that info by looking at where random cases may have picked it up], this may be why we’re seeing so many people active in the community.
It’s not 100% their fault. They just didn’t know they were infected!
I’m not a public health expert, I have some relevant qualifications though. But I’m not saying we should rely on rapid antigen tests either. We need regular old, highly reliable PCR tests too. The key to Iceland’s success is they also follow up on people.
The only restrictions they’ve imposed happened very recently – to outside travellers. This strategy worked so well for them, they literally had open borders and beat back COVID every time!
I dunno about you – but I wanna fish sooner. I wanna go back to med school, knowing I’m a little bit more safe, I’m sure you wanna work too. This is a hypothesis, but something we should consider at least! Comment your thoughts below. And subscribe to my email lists to get updates on this and to keep learning.
So recently, this document is being shared around by antivaxers created by a group called ‘Physicians for Informed Consent.’ The name is designed to garner trust, even though many, if not most of their members, are not physicians at all. They claim they’re not antivaxers to seem like they’re “only promoting safety,” making themselves out to be heroes, not grifters in this pandemic. They are in coalition with several anti vax organisations, and regularly make false claims and this article debunks them thoroughly and well (indeed, they are a well known quack coalition). Unfortunately it just goes to show that even qualified people see that there’s money in spreading misinformation, and make the calculated decision to ruin their reputation, and risk their licences to practice, against the money and influence they can get by spreading misinformation.
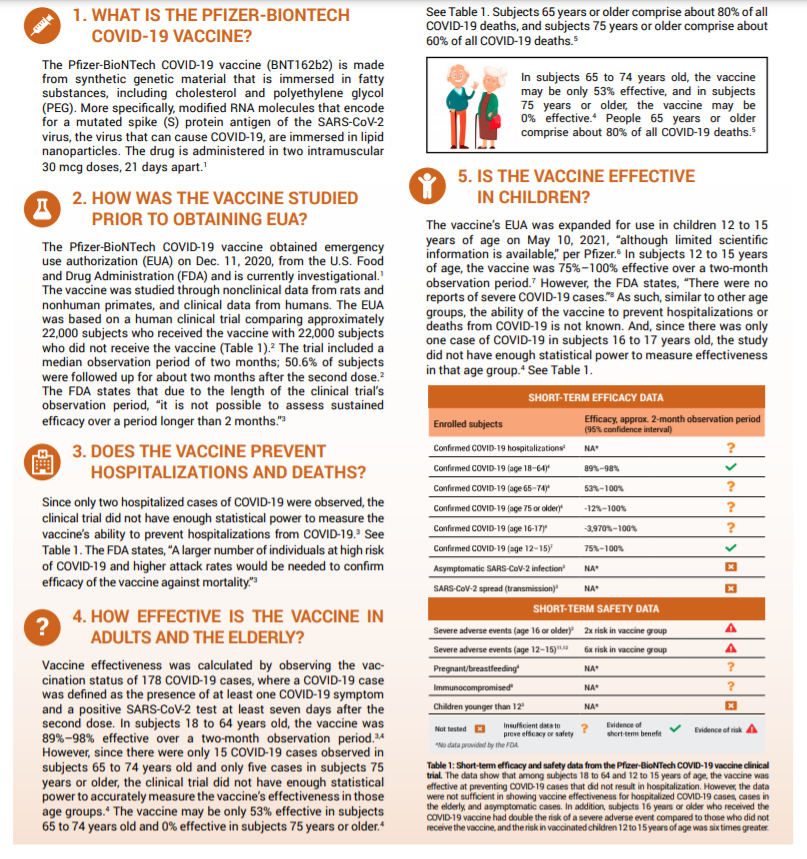
2) “The vaccine was approved early. It did not show long term efficacy.”
Yes, it was approved early, but this was due to it being an emergency. Significant data on safety had been gained prior to this, and efficacy was demonstrated to be very high through a trial with rigorous design, and COVID had killed hundreds of thousands in America alone to this point. There’s a reason this provision in FDA regulations exist. We are still collecting data on long term efficacy, but it’s been demonstrated regularly that long term immunity is formed after COVID-19 vaccination[1, 2].
3) “You didn’t get enough of a sample size and some age groups weren’t sampled.
So this is the thing. Vaccine studies don’t even need that many participants to get statistical power to make an apt conclusion. This study had MORE than enough (you need 10-15k to get statistically significant results typically). COVID-19 vaccine studies that led to Pfizer getting emergency approval had over 20,000. To this day, 4.5 BILLION DOSES HAVE BEEN ADMINISTERED to 31% of people in the world! This is no longer an experiment.
The fact that only 2 patients in younger groups got COVID doesn’t mean it’s statistically insignificant, it means the vaccine is very effective. You compare the numbers in both cohorts, and see how much of a reduction there is to calculate vaccine efficacy. So that part too, is wrong. In later ones they make further claims about lack of vaccine efficacy,
This study on the 2018 influenza vaccine enrolled 10,000 people. This one did 3600. That’s more than enough. If anything this had even more proof than most. It was approved for emergency use due to there not being long term data on efficacy. Safety wise, vaccines are very largely very very safe.
4) “This is NOT shown to be effective in older adults.”
You could make that argument as mainly younger patients were included in this study, but since the approval, we’ve gained a lot of data on this. 156000 patients over 70 were studied in this BMJ trial that showed 95% efficacy. This review found similarly high results.
Subsequent studies on this exact age group cited as a concern by this group of ‘physicians,’ (12 – 15 year olds) show very high efficacy of 100%.
This is not being seen now as we see many younger patients being infected with the delta variant. 30-40 year olds have 4x higher risks of death compared to 18 year olds. This is affecting more young people, likely because vaccination rates are not as high in these populations. And the delta strain seems to be more dangerous. So vaccinate!
Transmission reduction data against the delta variant is now available. Studies show efficacy against transmission ranges from 50 – 78% – against delta.
But you know what is very effective in reducing transmission of viral illnesses? Masks. See my blog post/mini review on them I posted earlier.
https://www.bmj.com/content/374/bmj.n1960
7) “Serious adverse effects are high.”
Serious adverse effects – they included things like muscle and joint pain, which occurs in 25% of patients and 17% of patients. Pain does suck, but it’s highly subjective. Other events included and mentioned first like diarrhoea and vomiting. Diarrhoea occurs in 1/10 COVID patients by ways of comparison. 0.07% of patients vomited after vaccination, 0.12% got diarrhoea (1/1000 or so). The source they referenced for this was a Pfizer vaccine trial’s clinical protocol which has no results, so I’m not sure where these numbers even came from.
We know incidence of things like myocarditis due to the vaccine are 1/100,000, and 0 deaths occured from this over 2million vaccines.
Finally, they end this suggesting vaccines are more dangerous than COVID in young patients, rehashing data they’ve made from invalid assertions earlier, that have been proven since in numerous studies done on young people, and old people. Long term safety data on vaccinations weren’t available then, but they are now. Long COVID studies are coming out though – and the consequences are dire. Studies show that 60 days after infection, 87% of people still had a COVID 19 symptom, with 55% having 3 or more. Scarring is present in the lungs of many. 20% of people hospitalised – which with delta, we’re seeing is occurring in younger patients – have permanent pulmonary fibrosis. Over 70% who are ventilated show this after 4 months.
Ultimately, we know this disease kills the unvaccinated more than any other groups – 99.5% of people who have died are unvaccinated. It’s not only killing people directly, but also people like me who are at risk, and need things like oral cancer biopsies (which I can’t get here in Aus as elective procedures are shut down).
https://www.forbes.com/sites/jemimamcevoy/2021/07/01/995-of-people-killed-by-covid-in-last-6-months-were-unvaccinated-data-suggests/?sh=6daccc9f493d
So yeah. 14 days ago now, I found out, in hospital I had diabetes. We went in for super high fat levels. Turns out it wasn’t the kebabs, but high blood sugar causing this. I was hoping it would be steroid induced. I just vlogged about it here:
But I have a LOT of questions that I guess only patients can answer. The little, tiny things – like:
1) Where and how do you prick (for insulin and blood glucose monitoring) EXACTLY to minimise pain?
2) Got any ideas of what things I can eat? I’m low carbs AND low fat.
3) I went really low, blood sugar wise, after exercising a chunk the other day. Even when I’m on insulin, how do I manage this? Should I keep some #gatorade or #jellysnakes at all time and take them when I’m feeling tired?
4) I’ve got a severe autoimmune-like disease, how do I tell if I’m hypo, or just having a bad day, or flare up?
5) Any devices or recommendations you can make for this all?
6) Is there an app for all this (the blood sugar app is OK, but like what works for you guys)?
7) Any good resources? Anyone I should follow with this?
8) What are your anecdotal experiences of medicines etc? (Don’t give medical advice in the comments, but do share your personal experiences!)
But I’ll try and share as I learn as well, because though I thought I got it, there’s so many tiny things that are confusing with this disease. But I’m getting there. One thing I’ve been doing – I’m cooking a lot now. And it’s been fun, being able to cook without cutting myself and feeling tireder after a meal (since my cramps are a LOT better). I’ll share those recipes too, because they’re actually so good! #Diabetes#T2dm#Diabetic#newlydiagnosed#spoony#chronicillness#newdisease#spoonie#cancerlyf#lol#medicine#doctor#medschoolSee Less
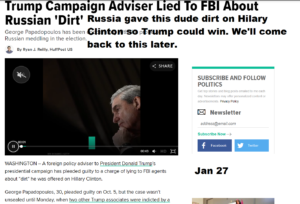
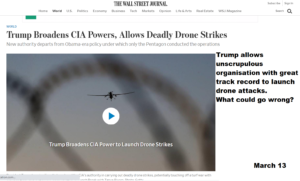
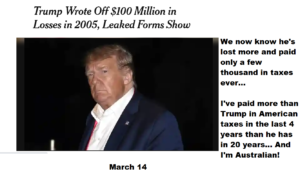
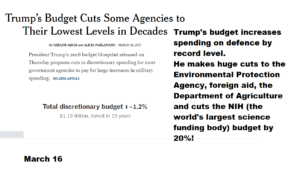
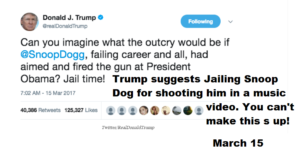
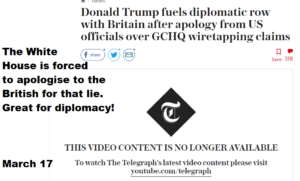
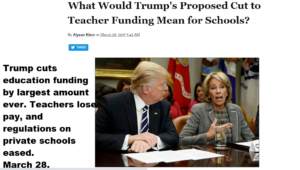
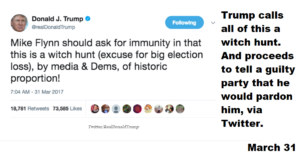
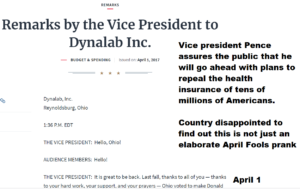
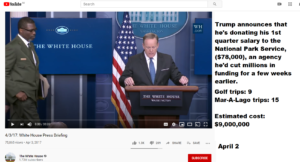
OK so I put together a video outlining Trump’s corruption and comparing it to Biden’s alleged corruption. The difference between the two is quite remarkable.
Trump golf count; it only calculates the cost of travel, by the way. The actual charges Donald charges his own hotels for his trips (which is quite high) is equally astronomical.
https://trumpgolfcount.com/QD
Ivanka Trump’s brand that was promoted by the press secretary.
Trump leases his own officer for $2.4million from 2017 – 18
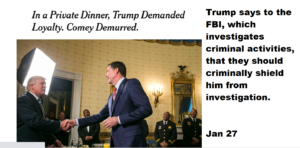
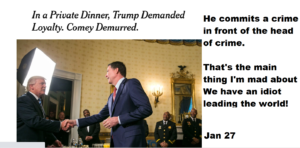
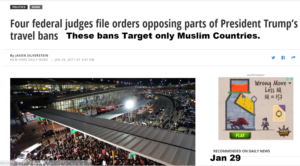
Welcome. I’ve lined up all the links to all of these stories if you want to reference them here. There’s a brief description and then the link for all the stories seen in the video. If you’d like to sign up to my newsletter so you don’t miss the next one – click here.
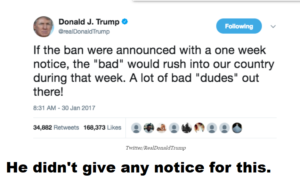
Fires James Comey, head of FBI, who was investigating him for colluding with Russia, and then the next day, divulges information to Russian Ambassadors.
Trump’s chief of communication calls random reporter and unleashses tirade on him. Reporter does the most obvious thing a reporter would do and reports it.
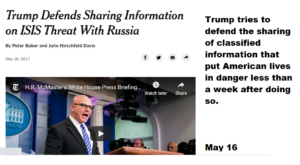
Recently, someone who follows this blog commented that they had no compassion for patients, and that this improved patient outcomes. It sounds heinous at first – god – someone like this in our profession? But he felt that there’s genuine merit to this idea. I know that at the very least, he’s a good nurse too. It was in response to a post I made on Twitter – below. He essentially asserted, and maintained after discussing with others, that he believes he delivers better care than others by not being compassionate, and focusing on evidence based care. It made me wonder, what is the actual evidence regarding the relationship between empathy/compassion and patient outcomes in healthcare.
It reminded me of a blog I read a while ago (I just can’t find it though!), of a doctor who said that in his department – emergency – they treated medicine like a job, as opposed to a service. And that this attitude led to lower levels of burnout.
So when he suggested the better option was his – apparently providing “more evidence based care in less time,” because he wasn’t spending time caring for patients, I dug into the evidence. This was my response;
“Yeah no, L. There is a dearth of evidence showing that patient centered care, which involves, heavily, taking care of people’s emotional needs as well as physical ones (for instance, ensuring physical comfort is maintained is important too), not only improves patient satisfaction, and reduces costs – but reduces mortality, and increases likeliness to come back and interact with healthcare too. Especially for those who are homeless (a population he prides himself on delivering better care to).
It doesn’t have to be a lot, or take heaps of time. There’s been recent support behind the 40 seconds of compassion model. But the “evidence” you say you put into your care, is just coldness. Other nurses and doctors ALWAYS practice with evidence too. They just do it better because they care as well. You think you’re a great nurse. You may be a good one, but you’ll never be a great one. Ultimately, the aim of healthcare isn’t to please or be liked by your peers or bosses. It’s to deliver good healthcare to people, and make sure people are happy as well. You can certainly do both by just doing your job, that is true. But you can’t confer the maximum benefit which leads to happiness and better outcomes.
A Ted Talk I’ll be watching tonight! The paper on this, I have read, and is linked below.
Having said that, there is an association of between burnout and poorer care and increased mortality. But distancing and detaching isn’t the fix – it’s actually associated with much worse rates of burnout. In some people though, they may have lower rates of burnout by detaching, you’re right. You may well be one of those cases. But you judging others who care as “wasting time,” when in fact, statistically, it’s shown YOU’RE wasting more time and resources, and contributing to worse outcomes by not giving as much of a damn as others, is 100% not fair.
I happen to agree that this cultural norm that seems to be propagated amongst physicians and nurses of ‘sacrificing for the good of the patient,” is probably taken too far by many. I know many doctors do suffer unnecessarily because of that, and some likely do burn out because of that. But the answer isn’t to detach – which creates EVEN MORE detachment, but rather to take time to care for yourself. If you’re happy and helthy yourself, you can give more of yourself, ultimately.
You do you – you may be one of the health professionals for whom not being compassionate may result in better care.
But don’t think you’re superior to others for it. According to the evidence, and likely from the patients you care for, you’re actually worse.
An excellent summary of the evidence showing patient centered, compassionate care results in better outcomes is in this paper – but I’ve linked several more for you to peruse as well. If you really care about evidence, have a look.
A report on the benefits of patient centered care – a model that advocates you involve patients in their care decisions, and that you provide both physical and emotional comfort to patients.
“Other benefits associated with patient-centred care include decreased mortality, decreased emergency department return visits, fewer medication errors, lower infection rates, higher functional status, improved clinical care, and improved liability claims experience.
In the care of patients with chronic conditions, studies indicate that patient-centred approaches can improve disease management; increase both patient and doctor satisfaction; increase patient engagement and task orientation; reduce anxiety; and improve quality of life.
Patient-centred care can also increase efficiency through fewer diagnostic tests and unnecessary referrals, and reduce hospital attendance rates. A patient-centred care approach has been linked to improvements in long-term outcomes in cardiac patients. Patient centred care is therefore regarded as an integral component of preventative care.
Increasing patient satisfaction through patient-centred approaches also increases employee satisfaction, and this, in turn, improves employee retention rates and the ability to continue practising patient-centred care.According to Charmel and Framton, the link between patient satisfaction and employee satisfaction is reflected in the fundamental philosophy of patientcentred care: the importance of staff feeling cared for themselves, so they can best care for their patients.”
More papers showing the benefits of compassion are linked below – including the largest systematic review on the topic. But I also believe, as you may have seen from the original Tweet above, that compassion and caring for patients isn’t an inherent trait that can’t be taught.
I believe it can and should be taught and mandated. Med school, or nursing school for that matter, is the best time to do this.
Me in my first clinic day of second year medicine!
“I was super shy and awkward in my first year of med school. A mixture
Reduced mortlaity even in myocardial infarction when more compassionate care was received – https://pubmed.ncbi.nlm.nih.gov/20662947/
Lowered pain, reduced anxiety, and faster healing, as well as higher likelihood of following care plans: https://www.novanthealth.org/healthy-headlines/the-healing-touch
https://pubmed.ncbi.nlm.nih.gov/15907021/
Just 40s of compassion resulted in better patient satisfaction.
https://pubmed.ncbi.nlm.nih.gov/10458256/
The largest systematic review found that burnout was negatively correlated to empathy. There are some studies which concluded the opposite, but they weren’t as high quality, and were in the vast minority.
In most studies – detachment is actually A MEASURE of burnout levels; https://www.researchgate.net/publication/260873755_Exhaustion_and_Lack_of_Psychological_Detachment_From_Work_During_Off-Job_Time_Moderator_Effects_of_Time_Pressure_and_Leisure_Experiences
It’s not compassion, but harder working conditions that’s related to burnout.
As it is Christmas today, I thought I’d share the best gift I’d ever gotten.
You see, in hospital, while getting my treatment (i.e. chemotherapy and radiation), I’d often wake up with intense pain or nausea, often finding myself drenched in sweat. And every time that happened, I got scared.
But the worst thing about that was that I’d wake up in the middle of night and not know whether I’d had 5 hours or 5 minutes of sleep… not know whether the doctors or blood collectors would be coming in soon, giving me ample time to sleep, or if they were hours away.
I couldn’t help but panic when that happened.
I used to always complain about this. But one day my uncle overheard me. And he thought up an ingenious solution for this problem.
He set out to get me a clock.
This is what he got me…
To this day, I can remember my jaw dropping as he unveiled this masterpiece. And never again did I feel that panic when I’d wake up at night. Instead I’d be left smiling at the most ridiculous gift I’d ever gotten.
The clock itself was a godsend. For the first time, I was lifted out of the confusion that is hospital, where I’d be stuck inside 4 walls, left to sit in a constantly chilled 24 degrees Celsius without any knowledge of what was going on in the outside world. I wouldn’t worry about whether or not I should bother to get back to sleep. I was, for the first time, in power in hospital.
But, to be honest, I think the best thing about this gift was the little thrill and that suppressed giggle I’d have every time a nurse burst into the room and said;
“My Nikhil! What a large CLOCK you have!”
Merry Christmas everyone.
Wish you and your families all the best for the next year, and hope this can help put a smile on you or your loved ones’ faces.