So masks are great. We should be wearing them when we need to go out.
But they don’t make you bulletproof.
I’m writing this because I’ve seen and been talking to a couple of very high risk friends, one who’s actively getting cancer treatment, the other halfway around the world, going out with masks. When I asked one – a friend who is on chemo (I was shocked that he was going to a stranger’s birthday party while Melbourne’s lockdown was going strong) – he said that did so because he’s wearing a mask, and that he should be fine. He’s either using a mask as a justification, or going out because of the mask.
It’s nuanced. It’s not easy to communicate, because we do want people wearing masks when they go out. But for years, its been suggested that we shouldn’t be giving people a false sense of security with mask usage[1,2]. The WHO didn’t make this suggestion out of the blue, as many on #MedTwitter suggest. Even studies modelling mask usage controlling the virus mention this[3].
There is evidence showing that this isn’t just conjecture too. This study used a location app to track individuals’ habits in mask mandated areas vs non mask mandated one. Those in mask mandate regions spent 20-30 less minutes at home, and more time in commercial locations directly after the mandates! It could be contributing to spread if there aren’t further measures taken by cities [4]. To be fair, this is a preprint, but unless it’s fraudulent, or sample sizes are incredibly small, a sharp drop in household days after mask mandates were given is telling. Perhaps it’s the mask mandates as opposed to the mask which got people to want to go out more. But that points to communication being an issue!
On the other hand, there is a review which suggests that mask doesn’t increase the risk of people going out that went viral. But though the medical world latched onto this, the study only showed that mask usage didn’t reduce handwashing. It didn’t (because frankly, it hasn’t been studied until recently), find if mask usage increased distancing[5].
I’m not saying that you shouldn’t wear a mask! The very opposite. Mask usage likely does reduce your risk of contracting a virus, and it IS definitively, through many studies, shown to reduce transmission if you happen to be ill in the community [7-9]!
But we should be telling people to wear a mask – IF You need to go out.
ESPECIALLY to those at higher risk. As many as 50% of the population in developed nations have a risk factor that increases mortality risk with COVID-19. There are many dying in their 30s. Long term complications are still not known!
If you’re at risk – Please, where possible, avoid going out if coronavirus is raging in your area. Listen to local health bodies and your doctors. That mask WILL reduce your risk most likely when you NEED to leave the home. And it can’t hurt you. But you shouldn’t be convinced that it will protect you. Even if you’re protesting a very good cause – if you or loved ones you interact with are at risk – I’d suggest you stay home.
The fact is – the WHO came out early on not recommending masks, as did many other nations, because the small studies that have been done on them show that in community settings – mask usage doesn’t reduce your risk of infection.
This RCT showed that it didn’t reduce your risk of catching disease significantly in younger populations[6] This RCT showed difference either – though its primary aim was to look at household transmission reduction, it showed that influenza like illness (a primary way flus are tracked) contraction was similar in mask/non masked groups [10]. They definitely DO reduce your risk of contracting illness, if they’re fitted n95s where users are trained in their use, as this review shows[7]. But that’s very different from community use.
Though countries like China and Japan are pointed to as proof of masks working, a study of Japanese mask usage has actually shown that it’s not masks, but rather the differing habits of mask/non mask users, that lowers their risk of contracting viral illnesses. People who wear masks tend to go out less, and wash their hands more than non mask wearing counterparts[11]. A similar study of Hong Kong residents found similar results[12].
But again, they definitely reduce your risk of transmitting disease to someone else, as I mentioned above[7-9]. And though statistically significant lowered rate of infection in these community studies wasn’t reached – you need up to 10,000+ people to get surveys like this to have statistical power (though this was an RCT, 1000 people to track a whole populations’ risk of flu may not be enough) – reductions in mask groups were seen.
Various lab bench/cough-simulating studies, like this one where outward particle emission was reduced by 90% on speaking[13], and common sense, we can tell that it will likely reduce your risk of contracting illness from droplets at the very least – even if it only stops you from touching your face as much[14]. But there are some studies disputing that masks even lower transmission with SARS-COV-2[15].
That’s why I emphasise, if you’re at higher risk – your best course of action is to stay away from sick people in the first place!
If you want to subscribe to an email list that’ll let you know if you can help scientists answer easy questions – check out CAroundYou.com/ProveIt
References;
I’m not gonna bother referencing properly as I’m not on my desktop which has EndNote, but should – I may later.
1) https://www.bmj.com/content/369/bmj.m2003
2) Culture matters a lot when it comes to mask usage and its efficacy. Really interesting look into this;
Recently, someone who follows this blog commented that they had no compassion for patients, and that this improved patient outcomes. It sounds heinous at first – god – someone like this in our profession? But he felt that there’s genuine merit to this idea. I know that at the very least, he’s a good nurse too. It was in response to a post I made on Twitter – below. He essentially asserted, and maintained after discussing with others, that he believes he delivers better care than others by not being compassionate, and focusing on evidence based care. It made me wonder, what is the actual evidence regarding the relationship between empathy/compassion and patient outcomes in healthcare.
It reminded me of a blog I read a while ago (I just can’t find it though!), of a doctor who said that in his department – emergency – they treated medicine like a job, as opposed to a service. And that this attitude led to lower levels of burnout.
So when he suggested the better option was his – apparently providing “more evidence based care in less time,” because he wasn’t spending time caring for patients, I dug into the evidence. This was my response;
“Yeah no, L. There is a dearth of evidence showing that patient centered care, which involves, heavily, taking care of people’s emotional needs as well as physical ones (for instance, ensuring physical comfort is maintained is important too), not only improves patient satisfaction, and reduces costs – but reduces mortality, and increases likeliness to come back and interact with healthcare too. Especially for those who are homeless (a population he prides himself on delivering better care to).
It doesn’t have to be a lot, or take heaps of time. There’s been recent support behind the 40 seconds of compassion model. But the “evidence” you say you put into your care, is just coldness. Other nurses and doctors ALWAYS practice with evidence too. They just do it better because they care as well. You think you’re a great nurse. You may be a good one, but you’ll never be a great one. Ultimately, the aim of healthcare isn’t to please or be liked by your peers or bosses. It’s to deliver good healthcare to people, and make sure people are happy as well. You can certainly do both by just doing your job, that is true. But you can’t confer the maximum benefit which leads to happiness and better outcomes.
A Ted Talk I’ll be watching tonight! The paper on this, I have read, and is linked below.
Having said that, there is an association of between burnout and poorer care and increased mortality. But distancing and detaching isn’t the fix – it’s actually associated with much worse rates of burnout. In some people though, they may have lower rates of burnout by detaching, you’re right. You may well be one of those cases. But you judging others who care as “wasting time,” when in fact, statistically, it’s shown YOU’RE wasting more time and resources, and contributing to worse outcomes by not giving as much of a damn as others, is 100% not fair.
I happen to agree that this cultural norm that seems to be propagated amongst physicians and nurses of ‘sacrificing for the good of the patient,” is probably taken too far by many. I know many doctors do suffer unnecessarily because of that, and some likely do burn out because of that. But the answer isn’t to detach – which creates EVEN MORE detachment, but rather to take time to care for yourself. If you’re happy and helthy yourself, you can give more of yourself, ultimately.
You do you – you may be one of the health professionals for whom not being compassionate may result in better care.
But don’t think you’re superior to others for it. According to the evidence, and likely from the patients you care for, you’re actually worse.
An excellent summary of the evidence showing patient centered, compassionate care results in better outcomes is in this paper – but I’ve linked several more for you to peruse as well. If you really care about evidence, have a look.
A report on the benefits of patient centered care – a model that advocates you involve patients in their care decisions, and that you provide both physical and emotional comfort to patients.
“Other benefits associated with patient-centred care include decreased mortality, decreased emergency department return visits, fewer medication errors, lower infection rates, higher functional status, improved clinical care, and improved liability claims experience.
In the care of patients with chronic conditions, studies indicate that patient-centred approaches can improve disease management; increase both patient and doctor satisfaction; increase patient engagement and task orientation; reduce anxiety; and improve quality of life.
Patient-centred care can also increase efficiency through fewer diagnostic tests and unnecessary referrals, and reduce hospital attendance rates. A patient-centred care approach has been linked to improvements in long-term outcomes in cardiac patients. Patient centred care is therefore regarded as an integral component of preventative care.
Increasing patient satisfaction through patient-centred approaches also increases employee satisfaction, and this, in turn, improves employee retention rates and the ability to continue practising patient-centred care.According to Charmel and Framton, the link between patient satisfaction and employee satisfaction is reflected in the fundamental philosophy of patientcentred care: the importance of staff feeling cared for themselves, so they can best care for their patients.”
More papers showing the benefits of compassion are linked below – including the largest systematic review on the topic. But I also believe, as you may have seen from the original Tweet above, that compassion and caring for patients isn’t an inherent trait that can’t be taught.
I believe it can and should be taught and mandated. Med school, or nursing school for that matter, is the best time to do this.
Me in my first clinic day of second year medicine!
“I was super shy and awkward in my first year of med school. A mixture
Reduced mortlaity even in myocardial infarction when more compassionate care was received – https://pubmed.ncbi.nlm.nih.gov/20662947/
Lowered pain, reduced anxiety, and faster healing, as well as higher likelihood of following care plans: https://www.novanthealth.org/healthy-headlines/the-healing-touch
https://pubmed.ncbi.nlm.nih.gov/15907021/
Just 40s of compassion resulted in better patient satisfaction.
https://pubmed.ncbi.nlm.nih.gov/10458256/
The largest systematic review found that burnout was negatively correlated to empathy. There are some studies which concluded the opposite, but they weren’t as high quality, and were in the vast minority.
In most studies – detachment is actually A MEASURE of burnout levels; https://www.researchgate.net/publication/260873755_Exhaustion_and_Lack_of_Psychological_Detachment_From_Work_During_Off-Job_Time_Moderator_Effects_of_Time_Pressure_and_Leisure_Experiences
It’s not compassion, but harder working conditions that’s related to burnout.
As it is Christmas today, I thought I’d share the best gift I’d ever gotten.
You see, in hospital, while getting my treatment (i.e. chemotherapy and radiation), I’d often wake up with intense pain or nausea, often finding myself drenched in sweat. And every time that happened, I got scared.
But the worst thing about that was that I’d wake up in the middle of night and not know whether I’d had 5 hours or 5 minutes of sleep… not know whether the doctors or blood collectors would be coming in soon, giving me ample time to sleep, or if they were hours away.
I couldn’t help but panic when that happened.
I used to always complain about this. But one day my uncle overheard me. And he thought up an ingenious solution for this problem.
He set out to get me a clock.
This is what he got me…
To this day, I can remember my jaw dropping as he unveiled this masterpiece. And never again did I feel that panic when I’d wake up at night. Instead I’d be left smiling at the most ridiculous gift I’d ever gotten.
The clock itself was a godsend. For the first time, I was lifted out of the confusion that is hospital, where I’d be stuck inside 4 walls, left to sit in a constantly chilled 24 degrees Celsius without any knowledge of what was going on in the outside world. I wouldn’t worry about whether or not I should bother to get back to sleep. I was, for the first time, in power in hospital.
But, to be honest, I think the best thing about this gift was the little thrill and that suppressed giggle I’d have every time a nurse burst into the room and said;
“My Nikhil! What a large CLOCK you have!”
Merry Christmas everyone.
Wish you and your families all the best for the next year, and hope this can help put a smile on you or your loved ones’ faces.
Nikhil Autar, Tumor Vaccine Immunology Researcher
Bachelor of Medical Research (WSU).,
Bachelor of Medicine, Bachelor of Surgery (WSU 2023).
Permanent Lung Damage is Almost Certain To Occur in Many COVID19 Patients.
Even mild infection can incapacitate healthy people for MONTHS.
It’s almost certain that COVID19 causes permanent lung damage in a large proportion of seriously ill patients. Young, fit and healthy people, including athletes, are not spared, and indeed, likely to suffer most (at the very least, they suffer for the longest). There’s a bit of evidence that those putting their body through extreme strain are more inclined to suffer worse outcomes when it comes to pneumonias. I felt my favourite stars, in my favourite sport, that I can no longer play due to severely damaged lungs, should know this information. Though important causes like the recent Black Lives Matter marches are indeed of concern, to both protect themselves, and the millions of young and old fans they have, it would be amazing if players could help spread this message – to distance, where possible, and do things like wear masks. Trust me – permanent lung damage sucks. I’m 26 and likely will never play basketball again.
Elite athletes are at higher risk of contracting COVID-19. Not only can exercise direct this particularly pneumo-toxic virus deeper into lungs, which may lead to higher chances of developing cytokine storms, and a more severe version of COVID-195, extreme exertion may reduce innate immunity, making players more prone to developing disease6. Not only is there this chance of permanent lung damage which could affect entire careers, It also appears that even mild infection commonly leads to a 20-30% decline in lung function that lasts for months12 – longer than the common flu – which could impact these very finals.
PLEASE – keep yourselves safe! Not just for your own sake, but also for others.
Many children follow sports stars religiously. Hopefully getting messages out to them and their families will keep, and the world at large, will keep them more safe.
It is concerning to see that sending children back to school is being encouraged by governments such as Australia8, against medical consensus. Opening up is occurring in the US too. Young people are similarly being asked to sacrifice themselves to attain ‘herd immunity’ around the world, athletes are being sent back into action. Though many are wary, as evidenced by Novak Djokovic’s diagnosis and disregard for social distancing, many aren’t spreading the right message, and may well be putting their teammates’ careers at risk.
It’s not to say we shouldn’t reopen. But we should definitely be encouraging safe habits like mask usage and social distancing – staying in unless necessary, or if public health bodies say it’s okay to – to minimize the damage. Not only to athletes’ careers, but to the world as a whole. This disease could be worse than we imagine. I just hope we can encourage eachother to stay safe.
I am an ex cancer patient, and extensive treatment has caused significant, permanent lung damage to me. My lung function is similar to levels seen in early studies of patients who were followed up after SARS-CoV-2 infection (a 20-30% reduction). I likely will never get to play basketball, or run, again. And though data as to extent of pulmonary fibrosis isn’t available yet, this data makes it clear that fibrosis is occurring. This is not something we want to expose multiple young generations to.
Zhang, P., Li, J., Liu, H. et al.Long-term bone and lung consequences associated with hospital-acquired severe acute respiratory syndrome: a 15-year follow-up from a prospective cohort study. Bone Res8, 8 (2020). https://doi.org/10.1038/s41413-020-0084-5
P Spangnolo, E Balestro, S Aliberti, E Cocconcelli, D Biondini, GD Casa, N Sverzellati, TM Maher, Pulmonary fibrosis secondary to COVID-19: a call to arms?, Lancet Respir Med. 2020 May 15, doi: 10.1016/S2213-2600(20)30222-8 [Epub ahead of print]
P Matricardi, RD Negro, R NIsini., The First, Comprehensive Immunological Model of COVID-19: Implications for Prevention, Diagnosis, and Public Health Measures, Version 1 : Received: 22 April 2020 / Approved: 24 April 2020 / Online: 24 April 2020 (10:25:27 CEST)
S Estruel-Amades, M Camps-Bossacoma, M Massot-Cladera, FJ Perez-Cano, M Castell., Alterations in the innate immune system due to exhausting exercise in intensively trained rats, Sci Rep 10, 967 (2020). https://doi.org/10.1038/s41598-020-57783-4
Bialek S, Gierke R, Hughes M, McNamara LA, Pilishvili T, Skoff T., Coronavirus Disease 2019 in Children — United States, February 12–April 2, 2020, MMWR Morb Mortal Wkly Rep. 2020 Apr 10; 69(14): 422–426.
Dong Y, Hu Y, Qi X, J Fang, J Zhongyi, Tong S., Epidemiological Characteristics of 2143 Paediatric Patients With 2019 Coronavirus Disease in China, Paeiatrics, Pediatrics April 2020, e20200702; DOI: https://doi.org/10.1542/peds.2020-0702
Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) — United States, February 12–March 16, 2020. MMWR Morb Mortal Wkly Rep 2020;69:343-346. DOI: http://dx.doi.org/10.15585/mmwr.mm6912e2
It’s been a wild year so far. So wild, I don’t even know if I’ll be able to tell the difference between an ordinary day and April Fool’s by what I’m gonna see on news and social media…
So much for 2020 vision.Can someone call it off, just for one year maybe? Be careful, and don’t be had this April Fool’s!
Be careful people. Don’t be tricked. If you’re keen for a laugh, check out this playlist I put together of the stupid stuff I’ve pulled on family/friends over the years!
So I’ve been getting a LOT of questions about COVID-19, the name formally given to the strain of coronavirus that’s on the verge of becoming a global pandemic. I’m particularly concerned that there’s a LOT of horrible horrible misinformation being spread, and many trying to profit off of this right now – including, but not limited to – pastors trying to convince people to drink bleach to cure non-confirmed cases of the virus. But it can be really hard to get proper information on this virus and how to prevent infection and spread. Hence, I’ve put together this blog post which I’ll update weekly every Saturday for the next few weeks (less and less frequently over time as or if the burden of disease diminishes).
Pictured here, your average Karen, freaked out by the Corona-virus. Should she, though?
How Lethal Is It? – More lethal than the flu, but numbers will likely change over time.
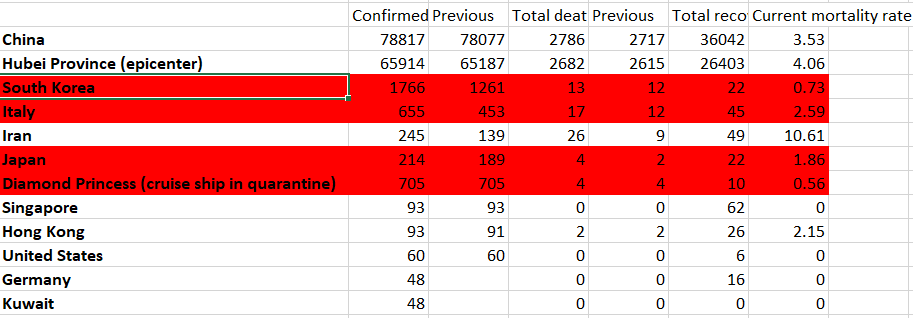
The latest information we’ve gotten directly from, largely, the Wuhan Epicentre (the numbers come from the Chinese Centre of Disease Control and Prevention) of disease shows that out of 72314 cases studied, there was an overall mortality rate of 2.3%. No deaths have been recorded in those aged 0-9, but deaths do increase exponentially with age, which is to be expected with many viruses of this type (peaking at a 14.8% mortality rate in those over 80). It’s important to note that an association with healthcare burden and death has been demonstrated in this virus, with the epicentre and neighbouring towns in the area seeing much higher mortality rates, which basically means, mortality rates could be inflated, as Wuhan exposures did dominate in terms of cases examined here. Poverty as well could skew mortality rates further as well, as is the case with many diseases such as measles. But figures may be downplayed as most cases of disease are mild, and the fact that China’s numbers and reporting of this has been questioned by many.
Important to note – Italy and Japan have both been ‘shocked’ by this outbreak and are now responding with vast restrictions, which should reduce incidence and cases. Iran, as you’ll see below, has not been following that example and has a notoriously bad health system to begin with, with some of the lowest number of hospital beds per capita in the world – fitting it directly under the low healthcare resources category described above.
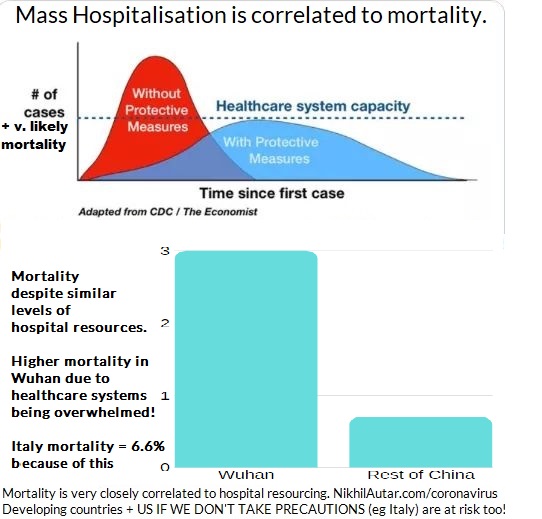
What does Flattening the Curve Mean, and why do we need to control disease early?
This summarises this best. But basically, the idea of making sure that both cases, and hence mortality, doesn’t exceed hospital system capacity is very important. As demonstrated above, there is a correlation between higher mortality rates and overburdened hospitals. Cases in Italy have been severe, to the point where doctors are being forced to make terribly hard decisions. If we stop the spread, however, we have the chance of not overwhelming hospitals and ICU beds and respirators, which are currently out of stock, and minimizing death.
I heard that China stopped the Spread. Can we do that too?
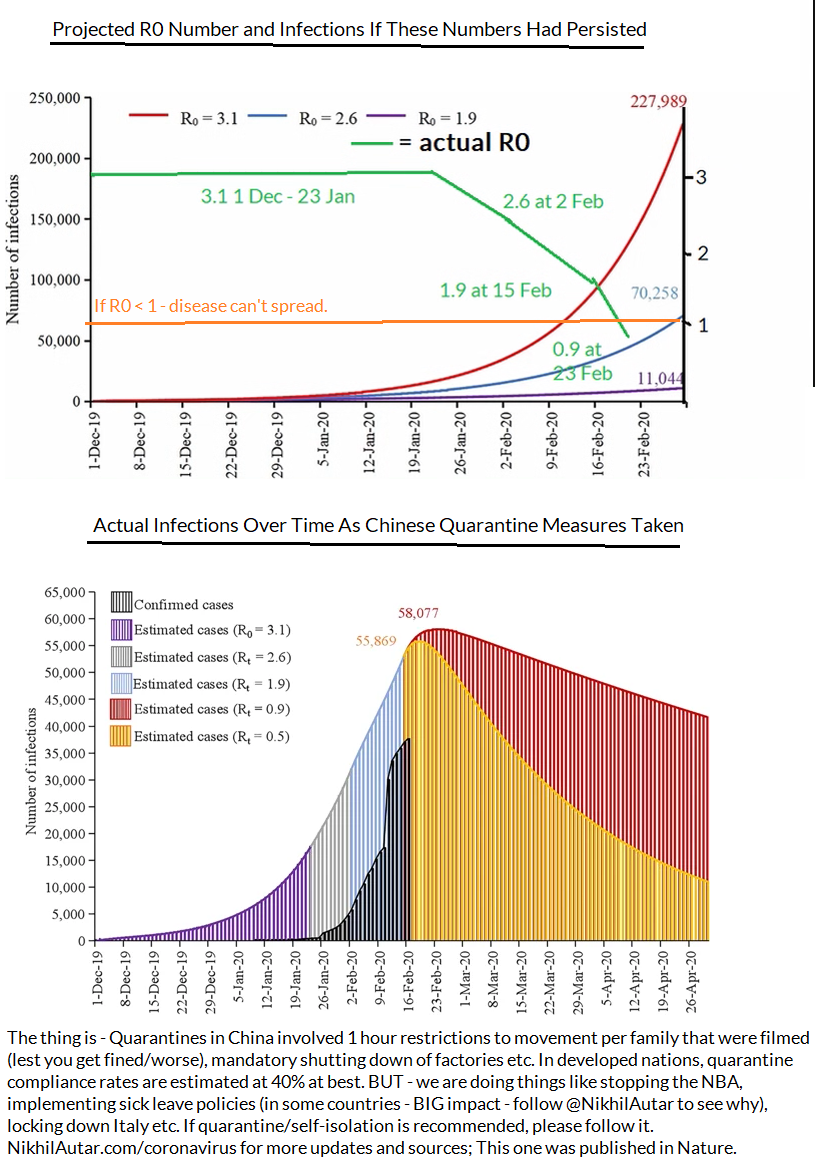
When the R Number reaches below 1 – disease can no longer spread. China has reached that point – but what remains to be seen if measures that Italy and other nations have taken can stop it in lieu of a vaccine which can help diminish spread or stop it altogether.
Outside of Age, are there any other risk factors? – Yes.
If you have preexisting conditions – the coronavirus could be especially dangerous for you, with mortality rates of 10.5% for cardiovascular disease, 7.3% for diabetes, 6.3% for chronic respiratory disease, 6.0% for hypertension, and 5.6% for cancer. It’s important to note that these diseases are often faced by older people and that these numbers weren’t adjusted for age in the study, but viruses do typically affect the already ill worse, so it’s very reasonable to assume there is a higher risk if you happen to fall under one of these categories.
How fast and far will it spread?
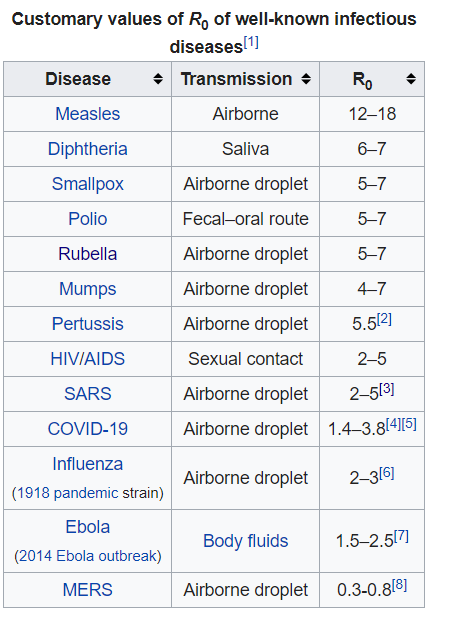
The “R Number” – R0 (the number of people you’ll infect, on average, if you get the disease) has been confirmed to be around 2.3, through a convenient study where 355 verifiably infected people managed to be in a confined space for a few weeks in a row – ideal scenarios for calculating this (which may, if anything, given it was done on members of a cruise ship which is REALLY confined) inflate numbers slightly. which makes it more infectious than the common seasonal flu, and even previous flu pandemics. It’s important to note though that these previous pandemics were in times when diagnoses weren’t high, and that other disease specific factors play into the spread, but though it doesn’t look high compared to other highly infectious diseases presented below – given disease characteristics and the lack of a vaccine, it’s definitely got pandemic potential.
Unlike the diseases ranked higher than COVID-19, COVID-19 does not have a vaccine developed for it yet.
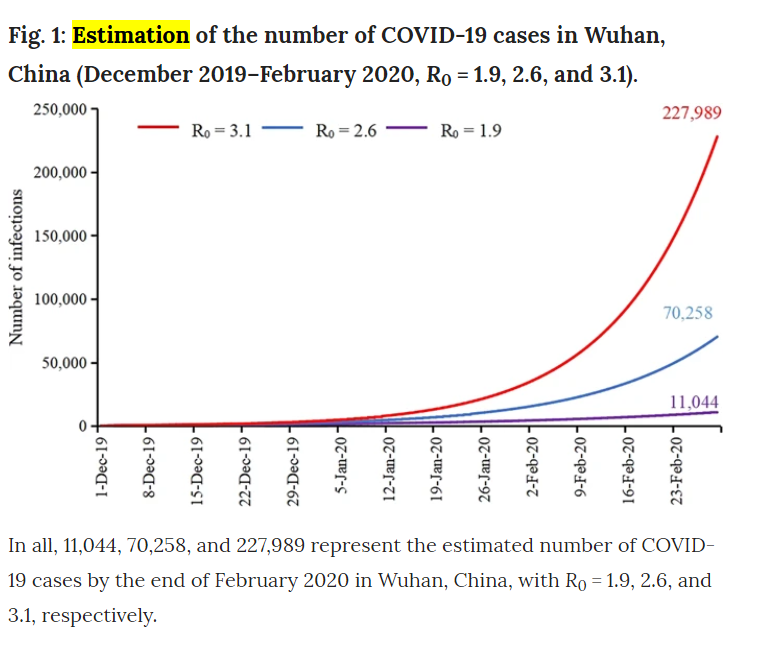
According to estimations made a few weeks ago (between January and Feb 15) on in the course of disease, there should have been less infections as there are now by the middling series of Rt estimates (in this study, they modeled data from January under projected number of cases and estimated that with a R number of 2.6, there should be around 70,000 by Feb 29. As of March 3, there are 80,000 cases in all of China. But with the interventions the Chinese government took, shutting down factories and effectively quarantining a nation, assuming a reduction in R0 as time goes on (which was observed by researchers), we should have peaked by now in terms of novel cases in this district.
Does that mean the spread is stopped? No – there were extreme measures taken in China and Wuhan in particular. But it could mean that R0 has been overblown thus far, likely due to endemic factors such as overburdening of healthcare resources, or poverty. We can’t know for sure right now – in any case, given its propensity to be more lethal
So what do researchers think is going to happen? Well, it’s hard to predict. But given that SARS and MERS, the 2 most recent coronavirus related pandemics we’ve faced, have been less community-spread than this strain of the coronavirus, and that there are numerous cases in the US popping up now where there’s been no contact between the patient and someone around them, there’s a higher chance of this spreading further than those other 2 did, but with lower mortality rates, it could be the case that this won’t be as serious. It’s great to see a coordinated global response behind this. But there are many instances of misinformation going around which is concerning to say the least. For example… it doesn’t help when thousands of pilgrims go around licking statues in Iran, the nation with the second worst outbreak of COVID-19, nor is it safe to go around, kissing people and making contact with random strangers in public, something the Pope insisted on doing despite Italy having the worst outbreak of COVID-19 (at the time of writing this) in the developed world.
Why? Surely Allah has better ways to test faith than challenging you to thumb your nose at what could be a global pandemic… As a nation which sees tens of thousands of pilgrims a day, and one already struggling to cope with the virus (indeed, it hasn’t got amazing healthcare, which, as we demonstrated above, is correlated to worse outcomes), it’s imperative we don’t do stuff like this.
Stopping Transmission And Reducing Your Risks
This is by far the biggest question I’ve gotten so far. Though some bodies are urging people to not buy masks and other personal protective equipment for the flu, mainly for supply chain reasons (practices in Australia are running low on supplies right now!), the evidence on whether or not coronavirus (or any virus for that matter), can be reduced in its transmission by things like masks or hand hygiene isn’t clear. There are several studies showing that transmission does go down with use of a more robust n-95 masks in healthcare workers who see this disease everyday. Medical masks aren’t shown to significantly improve rates of infection, but both treatment groups (those instructed to use hang hygiene, and those instructed to use hand hygiene and a mask) did see a reduction in rates of influenza compared to controls (yes, this was a highly reliable RCT, the only one I could find on this topic online). The facemask + hand hygiene group saw a 43% reduction vs 8% compared to controls with face masks alone, and none of the results were significant. But despite not reaching such large number, that same study ultimately concluded that these measures may help reduce rates of transmission, and that it should be recommended in crowded places during flu seasons.
Does that mean you need one if there’s no evidence of a major pandemic in your area? No. As there seems to be a global shortage – let those who need it most – healthcare workers who may be screening for this now – get their supply first if you’re well. But if you are a cancer patient, someone who’s got those comorbidities listed above (cardiovascular disease, chronic lung disease, diabetes or hypertension), I wouldn’t blame you for being cautious – especially if you’re going to hospital!
Finding a Cure
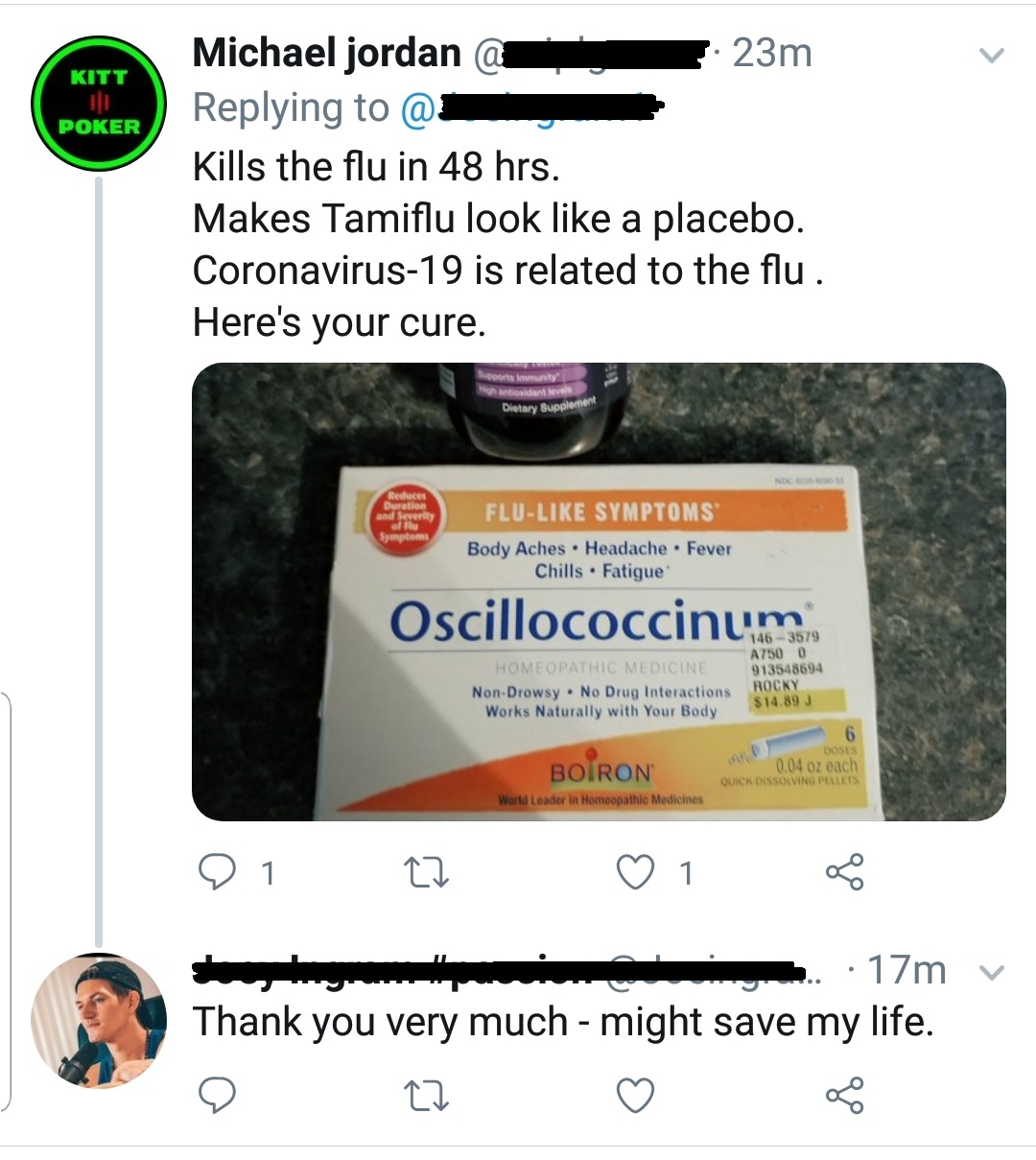
Another concern is media misinformation, and misinformation being spread by people on Facebook trying to make a quick buck off this epidemic. From that example of someone trying to sell bleach, to things you’ll see often in Twitter, or Facebook Groups everywhere, no – there is no verifiable cure for coronavirus yet. Research hasn’t demonstrated the virus is liekly to be susceptible to Tamiflu yet, but if you’re getting symptoms, and your doctor recommends it – take it. Though it may not be the easiest pill to swallow, it’s most effective taken soon after infection, and you could well have the flu which can be mitigated in its severity with Tamiflu!
Several homeopathic remedies have been suggested and are being sold to people on Twitter and in Facebook groups – don’t be fooled by the name. If it’s not being prescribed by a doctor, it likely won’t work, and you spreading that it could, could lead to people not getting seen by doctors, being diagnosed and properly quarantining themselves for one. Be very careful with what you say online!
In terms of vaccines, the world is responding rapidly. I saw my doctor on March 6, 2020, and he informed me there were 2 phase 1 studies going on, already, for the coronavirus vaccine. While it may not be included in the flu shot for Australia this year, it almost definitely would by next year. Phase 1 studies are occurring around the world. This one is estimated to be completed by September 2020, this one will start recruiting soon, and this phase 1/2 study will be recruiting soon as well. Several antivirals, including remdesivir, which was developed to combat the ebola virus, are also undergoing clinical trials.
Will the flu shot save me from getting COVID-19?
Donald Trump was recently reported to have asked why the seasonal influenza vaccine couldn’t be used to stop coronavirus transmission. Vaccines are targeted towards activating your adaptive, target-specific immune system. Basically, this response by your immune system relies on training, and facilitating the spread and growth of killer cells and ‘antibodies’ that respond to a particular, disease specific target. So vaccines targeting certain strains of influenza won’t result in cells that kill the COVID-19 strain of coronavirus. But in having said that, my doctor recommended I get the flu shot to reduce my chances of getting the coronavirus, as doctors are in my local health district. Why? Because, through various mechanisms, such as the release of factors which suppress immune responses, or the killing of cells which normally would block infections from taking hold through various mechanisms too. This study modeled the potential for flu vaccines to prevent SARS outbreaks through the reduction of influenza in hospitals, where these diseases tend to spread most, and spread most severely. We know that the flu, likely most severe viruses for that matter, diminishes your immune system and makes you more susceptible to secondary infections. Though these are usually bacterial, it is very much possible, especially when there are numerous strains of diseases with very different genomic profiles (making it less likely T cells that may have developed in response to one infection could eliminate a secondary infection with another disease), as is the case with seasonal influenza and coronavirus coinciding, for viral infections to occur after having had another. So make sure you get your flu shot people!
Another curious issue is the name of the disease. Thus far, the disease itself has been named COVID-19, and the international Committee on Taxinomy of Viruses is calling the virus itself SARS-COV-2. The WHO and this committee put out their naming declaration on the same day. The only actually published announcement I could find on “SARS-COV-2” was in a non peer reviewed journal, making me feel some researchers wanted to jump the gun and get a name for it first, But considering the impact SARS had in Asia about a decade ago, the fear it entails, and the propensity for this to be blown out of proportion by media outlets, given the previous SARS epidemic had a much higher 9.4% mortality rate, the WHO recommends using COVID-19 when talking about this – which is what I’ve done throughout this piece.
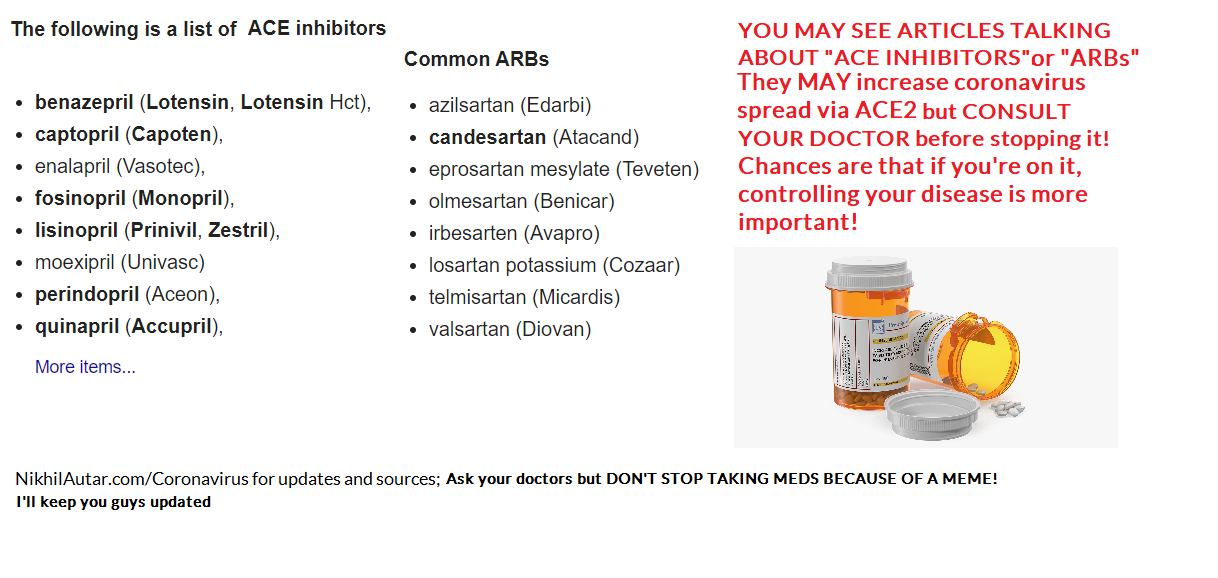
I saw something about ACE Inhibitors or ARBs (common heart drugs) being dangerous. Should I stop them?
There are some studies demonstrating the role of ACE2 in how caronavirus invades cells and spreads to cause disease. One study even speculates that these drugs here (angiotensin receptor blockers or ACE Inhibitors) may be the cause of such high mortality rates seen in patients who have cardiovascular issues as it is a commonly used drug to reduce hypertension.
But don’t believe what a few people are saying and summarily come off your medicines. Show your doctor these articles, sure, if you get the coronavirus, but don’t come off these drugs cold turkey without consulting your doctors because some guy on the internet told you to! Though in many cases, they can be substituted or ceased temporarily, some patients may NEED them to survive. Be very careful with information you spread!
A study demonstrating how ACE2 receptors allow coronavirus to enter cells where they replicate, infect further cells and create disease can be found here. Essentially, it seems like ACE2 is a prime way through which coronavirus gains access to cells’ DNA, where it can then replicate. This MAY be why therapies which drugs which target this receptor, which happen to be some of the most commonly used drugs in the world (as they’re used to treat hypertension, amongst other diseases), may be why patients are at such higher risk. There is a small number of animal studies which show that ACE Inhibitors may increase ACE 2 Receptor expression in peoples’ wind pipes, leading to more significant, potentially deadly spread. This BMJ study outlines how this is the case.
But THIS IS JUST A STUDY and indeed a hypothesis for now. The study itself highlights the fact that there needs to be further investigation into this. Stopping ACE inhibitors and ARBs cold turkey will definitely make you feel crap and could possibly lead to more severe side effects or disease outcomes, depending on what you’re taking it for. So don’t do this
Is it a disease that only affects the elderly?
It’s true, as I outlined above, that elderly people do suffer most, and comprise the vast majority of deaths due to COVID-19. But not only is there a chance of young people dying to it too, as is being seen around the world, numbers from the CDC suggest that young people are not spared suffering. 12% of ICU patients are 20-44, 20% of people in hospital with it are in that age group too. 9% of deaths occur in the under 65 age group. None of this is insignificant. As I outline here, ICU is one of the most traumatizing things. And there are numerous reports of permanent lung fibrosis, or scarring, occurring too.
Can Children (and Anyone for that matter) get Permanent Lung Damage?
Early on in this virus, doctors were making claims that fibrosis was evidence in the lungs of patients with COVID-19. Fibrosis is a scarring element that is permanent.
It is concerning to see that sending children back to school is being encouraged by governments around Australia, against medical consensus which suggests otherwise. Young people are similarly being asked to sacrifice themselves to attain herd immunity, but not only are there much higher rates of ICU admission and deaths being seen in 20-44 year old age groups when hospitals are overwhelmed, long term deleterious side effects of this through things like lung fibrosis is likely, and could have even worse economic outcomes in the long run too. Finally, sports leagues around the world, including our NRL, are also thinking about opening back up. With athletes in particular set to be severely impacted by lung damage, this should be taken into consideration too.
It’s not to say we shouldn’t reopen. But we should definitely not be looking to infect people to attain ‘herd immunity,’ not only because we’re not sure that proper forms of immunity will mount after infection (as opposed to vaccines which are optimized to create lasting infection – something I can explain further as a tumor immunology researcher), but because it could be much more dangerous than we imagine.
As someone who does have permanent lung damage of some kind due to chemo treatment, trust me, this is not something you want. I don’t know if I’ll ever be able to run again, yet alone do things like play basketball. You do NOT want this for your kids.
#DontRiskYourKids
What can you do to help?
Well the most effective organisation I could find, as judged by GiveWell and Charity Navigator (the number 1 and 2 evaluators of charities out there), is Direct Relief which is working with Chinese organisations and in the US and Carribean (and other places) to deliver money for research and PPE (personal protective equipment). That’s one way you can help.
Finally – the fact that there’s only been 1 study ever done on the impact of masks and hand hygiene on viral transmission rates globally irks me. My startup Centered Around You not only provides evidence based, AI powered wellness advice for the first time to general consumers, but also collects data in research friendly ways. Indeed, we have the potential to conduct a prospective follow up study, and more on this very task. Sign up for our email list to be kept aware of updates to this and to help aid research in this field.
And sign up to my email list to get updates on everything coronavirus and on other, mostly, health related stuff! I’m an ex cancer patient, current medical student, tumor vaccine researcher and founder of a few startups (to name a few things I do). I’d love to hear from you too! So check out my Facebook, YouTube, and Instagram if you’re there too!
So this all started from a Facebook discussion. Yet again, I found myself trying to reason with a brick wall of denial, conspiracy theories and anti-science, baseless rhetoric that is often espoused from the mouth of a “woke” hippy. Towards the end of it, as many who defend Alternative Medicine end up claiming, the lady I was talking to said, “The ONLY reason why there isn’t research for this is because BIG PHARMA can’t PROFIT from anything nAtUrAl.” And that from there, this lady went on to insinuate that 10million researchers and doctors, along with half or billion or so who work in health or health administration, were all in on a conspiracy to suppress the potential for elderberries to cure cancer.
Of course, she’d later go on to PM me her discount code, and an amazing opportunity to become part of an organisation that brings alternative therapies like those berries to the public, out of the Goodness of their hearts (it WAS only $99.99 to SIGN UP to the first pack which I could onsell to others – in other words an MLM scam). But by this stage I’d had enough.
Not only did it inspire this meme… It also got me to tear down her argument piece by piece.
Because pharmaceuticals, though they are HIGHLY unethical in their practices, unscientific themselves, and RICH as HELL – are not stupid.
And in the end, despite all their evils (and yes, I DO think many are just that), they, through the research and innovation they fund, ARE the reason we’ve got SUCH amazing healthcare, and why we’ve come SO far as a society, and species over the last century.
I mean think about it – if I came up to you, and asked you to give me $10,000 today… and that it’d take me at least 10, maybe 15 years to get it back to you… and that there’s a 94% chance you wouldn’t see that $10,000 ever again, you’d wanna get at least $1 million in return right?
Well, so do investors. That’s why laws are developed to allow a company that patents a drug and invests those millions into it, can set whatever price they want to and ensure themselves a monopoly – to allow for such expensive, time consuming research to occur.
That doesn’t justify them doing the abhorent, unethical things they do to sell these products though. Pharmaceuticals spent just 16% of their budgets on research and development these days compared to 30% a few years ago. They spend sometimes over HALF on SALES. And what does sales involve? Often, the most effective strategy to sell a drug, when it’s only able to be accessed by someone who’s trained to do so is to “incentivise” or pretty much, Bribe, doctors who prescribe medicines. There is ONE SALES REPRESENTATIVE (who are generally very well paid) FOR EVERY 10 DOCTORS in the US. That’s how lucrative this industry is – doctors are RICH. If you can invest that much into sales reps and turn a profit, that says something about the influence these untrained, not-necessarily-science-literate people have on prescribing practices!
The opioid epidemic IS something that’s been made a problem by ONE big pharmaceutical. And it’s resulted in over half a million deaths and infinitely higher rates of addiction in the US – and the family that facilitated it earned MORE from its sales than it’s being forced to pay out in fines. Though they may not get away with it entirely, I’m sure they’re praising themselves for making the correct business decision in doing so, the pure evil family behind this (John Oliver breaks this down brilliantly, here).
And because this industry is much more nuanced than anything I could go into in a singular blog post – not only because it’s healthcare, and everyone and every disease is different – but also for the rules and regulations that are involved in it… I’ve decided to just focus in on one issue that consistently gets brought up here.
The conspiracy theory espoused by many that Big Pharma is hiding the cure for it all. That this logistically could be done.
That companies or individuals would forgo opportunities to make billions of dollars to do so just to stick it to the common man (including their own family members)
And that pharmaceuticals are not able to, or not currently profiting from, therapies that come from natural alternative sources.
And in doing so, I’ll turn it back around. If it IS indeed possible to profit from supposed “miracle cures” that so many people swear by, is it more likely that there’s a huge conspiracy to suppress something that “freedom fighting,” “woke,” alternative practitioners and internet researchers are trying to dispel, or is it more likely that a $210billion, unregulated, complimentary/wellness/organic industry has a lot more to gain by spreading this kind of doubt, and profiting the easy way – by investing everything in fancy marketing and absolutely ZERO in actual research.
This is the actual trailor of “formidable mind” (formidable only because it’s one that’s never been used before) Gwyneth Paltrow’s new educational documentaries (obviously ranked less the lowest rung on the ladder that is the heirachy of clinical evidence), “Goop Lab.” I swear to God, the last 40 seconds is not edited in any way. That’s literally what they shot as a trailer. WTF?
So without further ado, here’s how I took on this hun trying to convince me, someone who’s written papers on the evils of the pharmaceutical industry (and who’s never been paid by them or given anything free by them) and how we can improve its efficiency, that there’s a HUGE conspiracy to HIDE THE CURE for EVERYTHING by, apparently, EVERYONE.
(She’d just linked me a documentary of I-can’t-remember-exactly-what to back up her assertions to contextualise things. This is something you may reguarly see from an irate me in the comments section of my Faeebook page – check that out if you have the time).
“Movies, memes and documentaries are not evidence. Hell, even what a doctor says is not evidence. It’s the lowest level of evidence and not recommended for use at all. Why? Because anyone can say anything. The benefit of science and evidence is that ANYONE can test and reproduce your findings to validate if what you’re doing is right. Individual practitioner experience is helpful in making decisions, yes, but we don’t use it for a reason. It’s what we did 1 – 2 centuries ago exclusively, back when our life expectancy was 40.
Without evidence, and indeed, big pharma, we wouldn’t have the drugs, quality of life, and life expectancy we have today – nearly 80 in most developed countries.
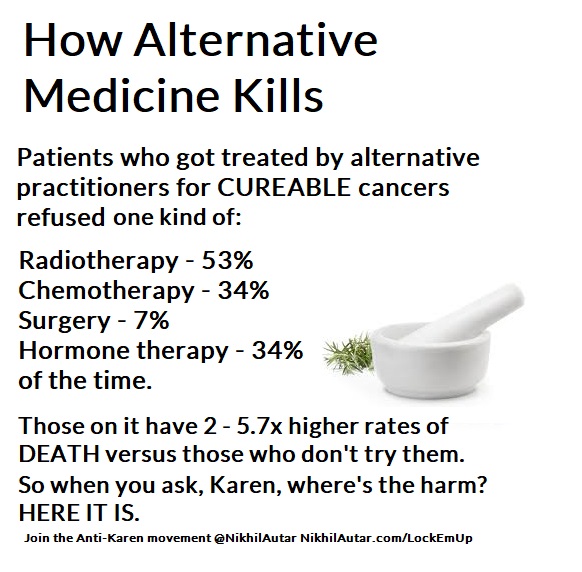
There are numerous, independent studies done on alternative medicines which show higher rates of death in patients who take them. These are patients who take them and avoid chemo and those who take them with chemo. It’s been shown that people who use alternative medicines are more likely to avoid sane, logical options for things that are shown to improve life expectancy, due to people like you, who spread misinformation. Some alternative medicines interact with and reduce efficacy of chemos (eg high antioxidant diets stop the effect of some chemotherapy regimes which use oxidation as a primary mechanism to kill cancer cells).
Why do some survive on alternative medicines though? Well,
a) There’s a chance it could be the alternative medicine. Indeed, we should study them too.
b) In many solid tumors, though, there’s a small to sometimes decent (depending on cancer, grade, lymph node infiltration, surgical outcomes etc) chance that surgery alone can cure it. Adjuvant chemo increases the odds of that immensely. Radiation post or pre chemo can too (similarly, some chemotherapies are given prior to surgery to reduce tumor volume to make surgeries more successful). So in some cases, some people do survive without chemo because of that. Likely, the ‘alternative medicine’ didn’t do anything there.
c) Some tumors also spontaneously remit – there’s a famous ‘wellness blogger’ who claimed her cancer was cured by wellness but who actually had a cancer which had a high chance of spontaneous remission is disgraced, and I believe, now sued because of this.
I talk about this, and how alternative therapies kill not only many who use them, but how they nearly killed me here – nikhilautar.com/lockemup
Is big pharma suppressing the cure? Well, you and many people don’t seem to know how the industry works, and how research works. Yes, there is investigation done into many drugs and natural remedies – a lot of blue sky research is done by universities, funded by government or by NFPs or collaborations between these bodies. But:
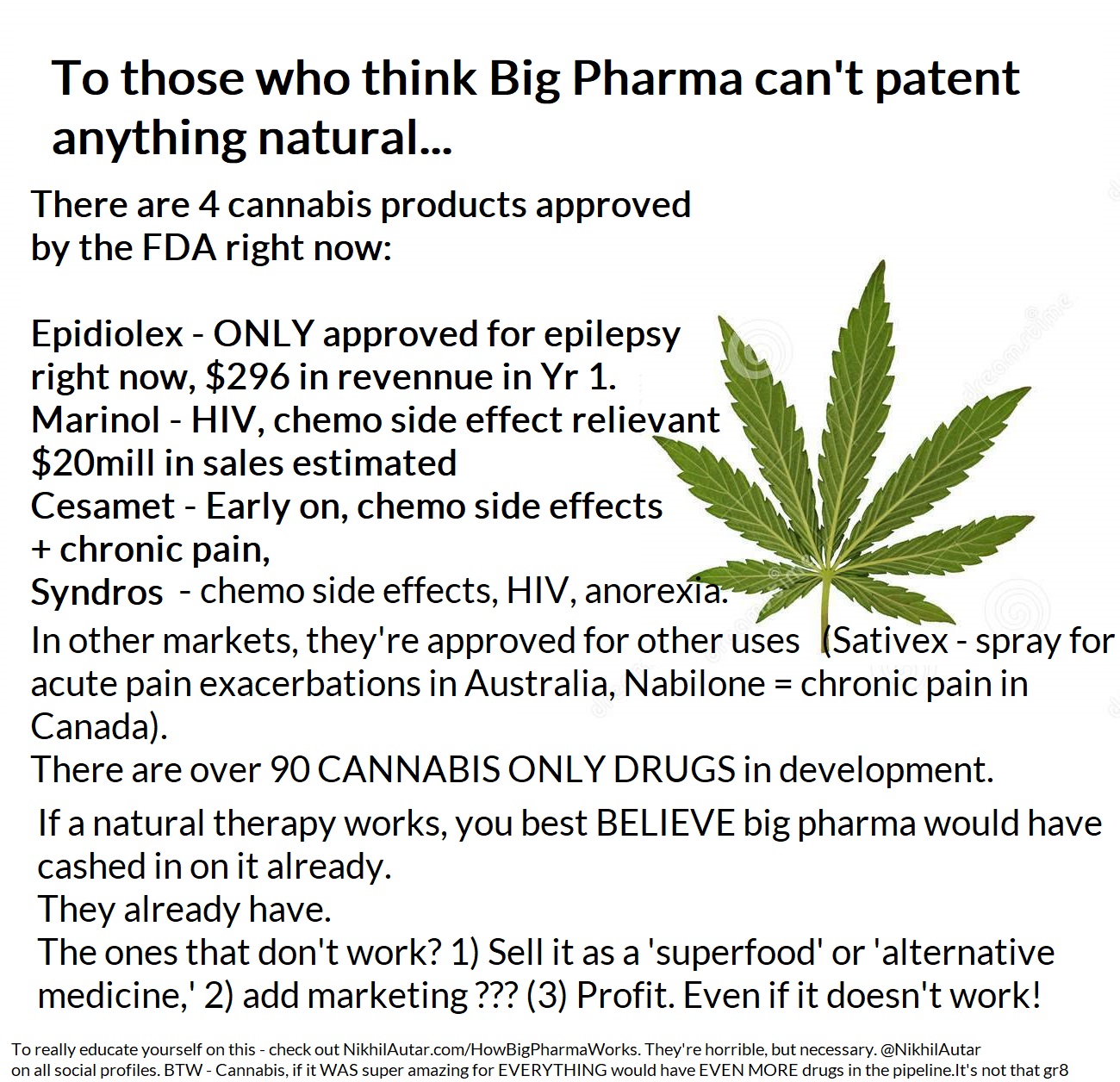
1) Big pharma, if they saw something had a relationship or correlation to success in alternative medicines, routinely will go out there and find a way to patent it and make BILLIONS from it anyways – even if it is ‘natural’. Contrary to popular opinion they can, and will make money off even “natural therapies” because their research and formulation is what the evidence shows and is approved by bodies like the FDA (and thus, the only legally available option of that kind for doctors to use to treat people).
Numerous drugs were traditional/natural/alternative medicines which have gone on to become multi billion dollar drugs. Paclitaxel (one of the most commonly used chemos), aspirin, various formulations of arsenic (used in some leukaemias) are famous examples of natural molecules they patented the manufacturing process of or slightly changed the molecule of, patented, and sold via sophisticated pharmaceuticals sales channels. Another example where they didn’t even change the original natural substance at all is marijuana. There’s a product which is called Sativex. It’s literally just marijuana’s main active ingredients in a specific formulation and given as a mouth spray that is now making tens of millions and will maybe make hundreds of millions/year but is no different to MJ. It’s just standardized and in a dosage and formulation they’ve studied and patented. Sativex is something my doctor wanted to use in me. So if it worked… big pharma could have and probably would have made money off it.
2) There are thousands – tens of thousands of companies at any one second developing drugs for various purposes as we speak. “Big pharma” isn’t just the big 5 – 10 companies which produce a fraction of the drugs that go through the pipeline. It’s a very competitive space. And though, yes, some of the big players are extremely huge, if there was something extremely promising out there, the tens – hundreds of thousands of small – large investors/venture capitalists/bankers out there who invest and often specialize in investments like this, would have jumped on it and made billions. Big pharma companies often just acquire these companies once they’ve done the hard yards, and use their extensive sales channels to distribute drugs that someone else has done the hard work/taken the huge risk in developing (only 6% of drugs that start phase 1 studies – the first stage of human trials – go on to be approved, in a 10 – 15 year process that costs millions to do, remember?). This isn’t always the case. Big pharma only invests 17% of their budgets into R&D. The rest goes into sales and M&As etc. Their tactics are highly unethical and I do hate big pharma with a passion for that reason too.
But without these big companies, we don’t get nearly as much funding for drugs, and we go wouldn’t be where we are today in terms of health outcomes. As recently as the 1990s, childhood mortality due to cancer used to be 85%. We’ve now flipped that, and childhood survival now sits at 85% in just 2 decades because of funded research.
While we’re talking numbers and feasibility, let’s also consider this… If there was such a conspiracy in place, whether it be in relation to vaccines, or “the cure to cancer” or chronic illnesses (because it’s not like there’s a huge shortage of patients to treat right now), you’d have to keep 10-15million doctors in the world, similar numbers of medical researchers, and between 5 – 7% of the world who are employed in healthcare, all of whom themselves have children/are likely to suffer from the diseases they’re supposedly trying to suppress, silent. No single company exists which could afford, and hide, $1000 in payments to each of these individuals. Though revenues (not profits – REVENUES) from the pharmaceutical industry top $1trillion, if you were to try and pay EVERYONE in this sector off, you’d spend at least half that in keeping people quiet IF $1000 would be enough to keep people quiet. With top doctors making millions per year… I don’t see how this could ever be possible.
3) There is already a LOT of research being done on various traditional/natural compounds on their ability to affect cancer. It’s not too hard or too expensive to do laboratory studies, which will be published in a journal somewhere if successful, and I know many studies are being funded through these pathways. Indeed, I have a few friends who’ve spent a year or two studying one or two in particular. My company will soon be automating medical research on consumers, and hopefully powering evidence based practice (sign up to help make this happen and win free stuff here) These (a) often haven’t been successful, or showed no results. As I said before, if they were so remarkable, big pharma would’ve pounced on them already, and (b) there’s a big problem in and of itself in that negative results often aren’t published, leading to people still insisting that things work, despite them being studied and showing limited to no success outside of early human, or petri dish studies. Petri dish, AKA laboratory studies, often don’t translate to clinical success.
Remember that 6% number? There’s many reasons for that – even a gun can kill cancer cells in a petri dish, you need to get the substance to the tumor cell, figure out how to administer it into a human body, make sure its safe and 1000 other little things to translate it into a successful drug.
It’s not as simple as “Hurr, durr, big pharma wouldn’t allow it” and “Big pharma is corrupt.”
The industry is VERY complex, but without it, we wouldn’t be where we are. Without medicines, we wouldn’t be here.
I talk about this more here. This is an essay I wrote looking into how we can continue to fund medical research in Australia which was shortlisted in an international essay competition (I believe it came in the top 5).
And yes – there is a chance a company will bury a drug that may hurt their sales overall etc. But remember also, there are thousands of companies around the world working on these problems, not just the top 10 which make up less than 1/3rd of revenues. That doesn’t mean they do 1/3rd of the research. The majority of early stage research is done by startups or small companies which will make loss for (you can’t make a penny until you have your drug approved) a decade until they get bought out by the bigger players, or raise a large amount to complete clinical trialing/start marketing etc their business.
So think more deeply before making rampant claims dudes. Because you don’t know who you’re hurting when you talk about something you know nothing about.
What are my credentials in this space? Well, not only am I a medical researcher who’s worked on a few clinical trial projects, and who’s written papers like that essay above on this topic, but I’m also the founder of a social enterprise which powers and may well automate medical research into this space.
Not only are we creating devices (something you may have heard me talk about on my various channels) that make life safer and easier for millions – something we’ve won innovation prizes and Australian Student Startup of the Year for in the past – we’re also connecting this to an AI powered app which I think has the most potential to create change.
Centered Around You, our app, will not only provide you with the most evidence based advice out there in the currently crowded, understudied (clinically at least) wellness space – in things like diet, exercise and sleep to start – but will also, through its inherent randomisation processes – collect large amounts of anonymised data that can prove if various interventions do measure up, and do what people expect they will.
Our devices, including our app, is something we’re developing to be medical devices that comply by various jurisdictions’ standards. They’re currently still under development, and in terms of the app and our first sensor devices, are currently being trialed in small user p9pulations – but we’ll need many more people to jump on board and make this a reality quicker for sure! Sign up to become a beta tester or to support at the bottom of the page on CAroundYou.com!
And do sign up for my email list to be updated of new posts on my blog too!
I should have noticed the red flags as soon as I saw that ridiculous logo and huge picture. I mean who starts a blog post off with a large, centred picture of some generic image, designed to drive traffic to your article, right?
When you dig deeper into articles that make bold claims like this though, you often will come across big issues.
This article cited just one medical journal article, which claimed “93% of patients would prefer cannabis to other drugs”, and that “81% of patients reported cannabis alone being better than combining cannabis with opioids” – those high numbers alone instantly screamed “red flags” to me. But upon deeper inspection, there were several more flaws in the study (linked here)
.
First off, a survey study, with no mention of HOW patients were recruited, any randomisation or other such checks or balances or ways of reducing bias destroys the reliability of such a survey completely. This could have (perhaps, it likely was) distributed through a series of pro cannabis pain groups on Facebook for all we know – which would obviously make all results biased.
There are validated pain scales, and better ways of studying the effects of treatments like this, like prospective follow up studies (if not RCTs) of patients who tried cannabis versus those who tried opioids. Though these are harder and more expensive to conduct, if doing a self reported outcome studies – which can still be quite valid (though it’s hard to do this when retrospective) – the authors could have used many techniques to make their findings more solid. They didn’t.
And though the journal this article was published in is peer reviewed, its CiteScore (similar to journal impact factor) is 3.1 – which is quite low – and definitely guilty of publication bias from the quick inspection I did of its most recent titles.
Cannabis is an interesting drug. It DEFINITELY has amazing impacts and potential to help A LOT of people out, likely with less side effects and more efficacy than current treatments for sure! But it also has a cult-like following of #woopedallers who overblow its ability to cure ANYTHING AND EVERYTHING just because it’s #NATURAL and #DANK too.
I did a quick literature review of the matter, going into it thinking, if anything, that medicinal cannabis’s most commonly studied compounds, CBD (cannabidiol, a non psychoactive compound that acts on cannabinoid receptors in the body), and THC (a psychoactive compound that also works on those receptors -the video below is a good summary of the body’s endocannabinoid system), would help in chronic pain with minimal side effects, or at least not be harmful. Please note, I focus on CHRONIC pain. Because that’s where it’s been studied, and used, most.
A general view held by many (not just ‘potheads,’ but doctors as well) is that MJ is not too harmful. But there are certainly side effects that need to be considered. And the results on marijuana’s efficacy were surprising to say the least, as well.
To summarise, it seems THC, the main compound used to treat chronic pain, seems to make pain more bearable in some, but given its ability to cause mainly psychiatric side effects (including exacerbation of pain, the very thing we’re trying to treat, anxiety, and the activation of psychoses), caution and further research must be done to validate its use, and use cases.
In chronic pain – this great review (reviews are the highest qualtiy, most reliable studies we can get, as they gather data from numerous great sources) goes into the fact that compared to opioids, cannabis based pain treatments actually caused more side effects than opioids per person treated, with a number needed to harm (the number it takes for a medication to do something) as low as FIVE in patients being treated with cognitive issues, while showing no evidence of superiority to opioids either.
This study actually showed cannabis use made chronic pain WORSE in most people who got them – AND it was associated with a higher risk of anxiety too! They didn’t even reduce opioid use!
Now again, these studies are mostly describing associations. Marijuana is often used as a self medicating tool by people with trauma, or who are going through tough times. – these studies are often describing associations. But there is likely a causative element too.
Contrary to popular opinion, you do develop withdrawal symptoms when coming off marijuana (dependence) – with patients experiencing symptoms 24-48 hours out of cessation (it can last up to 3 weeks, but usually is bad for a week). Though not as addictive as other drugs, it can indeed induce cravings too (addiction).
Despite claims it’s “100% safe” and that it “never kills anyone due to overdose ” (deaths due to overdose are indeed very hard to induce via cannabis), almost 350,000 people enter EDs every year because of cannabis for various reasons (from anxiety/panic, to seeking help for addiction – which accounts for over half of these – 177,000 presentations per year).
Now for many, if not most, marijuana is perfectly safe. But I point these out because so many believe, and espouse to the world that it is ‘completely harmless,’ when that’s definitely not the case.
Some suggest that cannabidiol (aka CBD), one of the major MJ-derived compounds used for medicinal purposes, which has a much lower side effect profile compared to THC (the other major MJ-derived compound that causes you to get ‘high.’), may improve pain, particularly neuropathic pain, without much in the way of side effects! But THC is the substance most studied in chronic pain thus far, and that does have higher rates of negative side effects (though some may suggest the psychoactive side effects aren’t negative. Often… it’s the point of the whole exercise).
Overall – Medical Marijuana is likely not a viable first line treatment option that we should be prescribing for pain patients in favour of other, less harmful treatments, like cognitive behavioral therapy, treating the causes of pain and other neuropathic/antidepressant medications. Opioids may help some who don’t develop tolerance, better too.
But that isn’t to say opioids, or #bigpharma are amazing either.
The opioid epidemic is VERY real and a direct consequence of a few pharmaceuticals going borderlinie LEGALLY rogue (they claim) while making wild claims about their drugs being safe, non addictive and effective (which was done completely illegally). Corrupt and/or negligent doctors WERE very much part of why this got out of hand and has resulted in mass spikes in opioid related deaths in America and other developed nations too. John Oliver explains this REALLY well in this video – but when a system exists where a single family can PROFIT despite paying billions in fines and breaking criminal law, and killing half a million people in the process… that’s just as bad, if not worse, than snake oils salesmen scamming people and taking lives in their own insidious way too. 1/32 people prescribed 200mg equivalents of opioids DIED during this overly salacious period of prescription. And today, as the government bears down on prescribing these drugs arguably too heavily (denying legitimate patients who NEED these drugs to function), even more are dying to things like suicide.
Lack of phaemaceutical oversight is something I’ll be calling out always – even if it loses me ‘fans’ or ‘followers’ – because that too is wrong. There is no reason pharmaceuticals should be allowed to use the tactics they are allowed to. Right now, they spend more than TRIPLE on selling drugs than they do developing new ones. Drug development is skewed too much towards profit these days and productivity/innovation is going down as less and less drugs are in the pipeline – it does need fixing.
I actually wrote a paper on this which never ended up getting published anywhere but did still place me highly in a national essay competition. You can check that out here –> https://nikhilautar.com/improvingbigpharma/
But another downside of opioids is its potential to be addictive, for patients to develop tolerance and/or withdrawal too. This is often overlooked by doctors. And perhaps that is where marijuana shines over opioids. Not for all. But certainly for some.
Sadly, chronic pain is also assocaited with high rates of depression and suicide. If you’re struggling with it, like I did, do seek help, and google crisis support lines if you need to (or better yet, if you have been feeling not the best- memorise them!).
I talked about my own experiences of dealing with withdrawal symptoms after coming off pain medications post surgery on my Facebook page – which you can check out by clicking here!
This is going to be a compilation of the top 1000 tips to keep you happy and healthy during hospital… one of the most dangerous and boring places in the world.
It may seem redundant, but believe me when I say this, the TINIEST little things in hospital can save you the most pain and struggle. Tiny things like this.
I’ve been in and out of hospitals for 8 years but only picked up this trick on this admission… what you see here is your hospital bed remote and your nurse alarm/TV button. Keeping things close at hand in an organised fashion is of HUGE importance.
I did used to use a side rail which I’d keep up to hold my bed remotes n place, but only a few weeks ago did a nurse suggest MAKING THE BED REMOTE FACE ME and hang it up that way for the first time. I can’t believe I hadn’t thought of this before.
But ESPECIALLY in this admission where I’ve been restricted from lifting more than 1-2kg at a time to let my chest wound heal, this tiny change has been LIFESAVING.
These may seem like nothing but they do add up. The other day, I was hooked to a non mobile (non wheely) IV pole and the nurse call remote was on the floor (plus, as I have for the last 3 weeks, I’ve been hooked up to a Vac seal dressing too on my left leg). And I REALLY needed to go to the bathroom.
Mum and dad just happened To be out. My phone wasn’t in reach either.
Instead of panicking and trying to twist and contort my body, which could risk my cannula falling out or even worse, result in me falling, I screamed out for a nurse for the better part of 10 minutes until 1 arrived.
A less patient, younger me wouldn’t have though.
Share this with anyone you think this could help.
If you have your own tips you wanna share or wanna see more – itll be here and on my Facebook page or on Nikhilautar.com/hospitalhacks . Tell someone you love, if they’re in hospital, to always have their necessary devices handy, and ready to go, where possible.
The same lessons apply for your bed side tray table. Keeping your laptop, devices, chargers or books there and in easy reach is a no brainer! But things like alcohol hand sanitizer, tissues, and water bottles should not be overlooked too!
Staying SANE in Hospital – Utilising all their services;
DOGTOR consults
When i visited a friend in a children’s hosiptal for the first time, I was jealous.
THEY BROUGHT HER A PAIR OF DOGS TO CUDDLE WHEN SHE WAS IN HOSPITAL!!! Children’s hospitals have and get everything it seems.
But you know what? Virtually all adults WILL have a therapy animal service available to patients.
Understandably, in some wards and for some patients, this isn’t ideal or suitable.
But I mean if you CAN – why NOT get a visit from a fluffball? They’re actually not too dirty. The germs and illnesses they have are not transmittable to humans and these dogs are tested regularly. And pet visits are shown to improve health outcomes for many.
But other amazing services I will be updating you on further and expanding on soon are:
Dietitians – they can hook you up with extra food, or whatever food you like, in fact!)
Occupational Therapists – who will help make tiny little adjustments that DO make your life safer and easier – and, depending on your insurance or where you’re from, perhaps even get you free stuff.
Physios – they are people you may HATE at the beginning. But consistent work with them during Rehab can change your life – especially early after your body goes through hell like chemo or surgery.
Psychologists – they’re always there in hospitals and always willing to listen. At the very least, they give you someone to chat to. In a time when you’d otherwise be bored, and surly… why not continue healing in the place that arguably makes most sense to work on – your mind?
So you guys may have seen this in your news feed recently, and I thought I’d give my $0.02 on it as a tumor vaccine researcher.
It’s pretty exciting stuff, always, to see innovations occurring but this kind of thing is something we’ve known and been doing or decades. There are several ways in which tumor vaccines work. The difference between them and traditional, preventative vaccines are that tumor vaccines are usually THERAPEUTIC. They basically try and create specifically targeted immune cells that target your cancers through using proteins, or bits of DNA or even just killing off whole tumor cells and hoping the immune cells that are generated from cleaning out this ‘tumor infection’ we created are primed to kill your tumor cells.
Often what cancers do as they develop is create a microenvironment that’s immunosuppressive – which doesn’t allow immune cells, even if they do infiltrate the microenvironment, to create tumor-specific responses. They do this via creating areas which have immunosuppressive cytokines everywhere around a tumor, and also by producing proteins (called checkpoint proteins, eg PD-L1, which cancer cells start releasing after a while, binds to various T cells to stop them from activating and killing cancers) which inhibit immune cells from attacking cancer.
A great video that summarises how Checkpoint Inhibitors, an exciting new development in immunotherapy, work.
What the flu vaccine in this case does is create an environment that’s the opposite – that’s suddenly immunogenic, where inflammation is occurring, bystander tumor cell death may be occurring and at the very least, where we’ve got less immunosuppressive factors, and more activation of your immune system, occurring right next to cancer cells.
This picture shows a few of the pathways that tumors use to dampen immune responses against them. The flu vaccine, it appears, can mitigate or reduce a chunk of these!
This isn’t the first time that viruses have been used to increase the immunogenicity against tumors. Various viruses, from Herpes in brain cancer, to Newcastle disease, are used to boost the efficacy of a tumor vaccine, and some have, like Herpes in brain cancer, been used on their own to enhance tumor cell death.
Indeed, I’ve written up the most recent review on how to use viruses, and numerous other strategies, to increase the immunogenicity of tumor vaccines. It’s yet to be published, but will be soon – look out for that (sign up to my email list and I’ll ensure you get a copy when I’m able to release it)! It’s fascinating stuff that I chose to work on because it requires you diving DEEP into the mechanisms underlying immune evasion by cancers and immunotherapy in general.
But though it’s great we’re seeing results of the flu vaccine working on its own – its potential to be combined with tumor vaccines is amazing. Whole cell tumor vaccines, which is the type of tumor vaccine I studied (they essentially kill off a person’s tumor – with radiation, electricity or other means – and reinject it back into your body to awaken your immune system to targets that are now clearly visible to the immune system), could definitely benefit from this boost.
The great thing about these therapies is the fact that similar to regular vaccines, tumor vaccines are often really well tolerated. Other than discomfort and swelling at the cancer site, and sometimes a few more systemic symptoms, most human trials show decent results with minimal side effects. But though this is true, the efficacy of tumor vaccines on their own is often not that great compared to other therapies.
So though this isn’t a HUGE NEW DISCOVERY – it’s still an awesome one to have been made, and provides just another reason for people to get their flu shots, which, as I talk about in this video ARE SAFE AND EFFECTIVE!