As many of you know, I’ve been preparing for this bike ride. And I’m glad to announce… formally, well, on this blog, that only 2 months after I was done with chemo, I managed to complete the Sydney 200km Ride to Conquer Cancer!
I was scared about it for months… But when I arrived at the start-line… just seeing so many people there who wanna beat this thing, hearing them encourage each-other on, and just immersing myself in the positive atmosphere took away all that fear.
I was pumped. And the ride’s excellent logistics, the crowds cheering us on throughout the ride, the other riders urging eachother up the hill and the people who approached me, telling me my speech brought TEARS to their eyes; that they were riding for ME… that kept me going.
And I made it =]
It was honestly, the best weekend of my life. Being cheered on every few kilometers on the track… inspiring and being inspired by so many other riders all there for the same thing… getting to hear from and talk to and help others who have family, friends, or have suffered themselves from this horrible disease… What more could I want from a weekend.
Everyone felt the same way. Whether it be on the ride, where everyone somehow had a smile on their face, despite the pain their legs and behinds were going through… Or at camp, where we’d rest and cheer the other riders as they shared they stories… Or at the finish line, where everyone, not matter how much suffering they were going through, would stand up and cheer the last rider on.
Everyone felt the same joy, the same feeling of accomplishment.
And it was because of riders like us that the Chris O’ Brien Lifehouse received $3.6million from the collected fundraising of 905 riders. And I remembered how every time I’d hear about a fundraising event, or a new breakthrough coming through to fix cancer while in treatment… I’d get a smile on my face. Not only did we raise a huge amount that may just change the outcomes of millions of patients in the future, the fact that we were all there to show our support put a smile on EVERY cancer patient’s face. And That’s AMAZING.
This was my speech to start the event:
My training schedule and the ride itself:
It wasn’t as hard as you’d think!
The ride was daunting. The number, 200 (120miles) – terrifying to me before it. But with a few months of gradual build up – the day actually wasn’t too bad.
I mean the nutrition we were supplied with, and that I brought on the day itself (and my preparation), made the first 80kms of each day not too hard to keep pumping. Except for the hills… where everyone’s encouragment and the crowds along the ride kept you going!
We did 100kms on the first day, camped out overnight, and did 112kms on the second. Everything was provided for – no worries there! And it cost only $50 to register. Honestly – just to have that experience itself would have set us back a few hundred bucks. It was very well run!
What I ate the day before: I followed the pro’s, and general marathon advice. I had wholemeal pasta, with lean meats and a regular-spicy sauce (to taste) of course =P
During the ride, the regular pitt-stops, every 20 – 30kms at the start, and every 10kms towards the ends of both days, had Shotz tablets; the brand of electrolyte the pros on the Tour De France drink (at $4 a pop, with multiple bottles drank on each day – that itself helped us keep going). We had protein bars there too, as well as lunch on both days – a good, carb-rich, lean meat packed wrap or sandwich (with vegetarian options also catered for of course).
At camp, we had pasta with some very nice sauces too. And we had massages provided, as well as family and some amazing speeches to sooth our sore muscles too. It was great, and by the next morning, I was repumped to ride again!
The training up to this ride was also great – because I built up slowly. As I said in my video – I could only hit 5minutes on the EXERCISE bike when I started, I was that tired from all the chemo. But over the period of 4 months, I managed to get up to doing 50kms comfortably. And when I went out and rode – the adrenalin, the amazing atmosphere and the expert, well rationed nutrition – that took over. And I did it. As did many others who were nervous about it too – including a 70 year old lady I was talking to who had a partner, the same age, who had passed even dad and I!
And training for next year will be even better! Because I’ve managed to recruit mates to do it with me! And I invite you to join me – feel free to reach out and train with me – or get your own group of friends, colleagues or family and get out there and help conquer cancer too!
This was pretty much a copy-pasted conversation I had with a friend asking for UCAT tips, so sorry if it’s not that well worded. In the time I did it – the UCAT was called the UCAT! But the principles, time sensitive nature of the test, and test taking skills are essentially the same. I figured I’d put up one of these so I wouldn’t have to do them individually any more and to help you guys out =P
For those who don’t know, the UMAT – now known as UCAT – is a challenging pre-medical test every prospective doctor needs to sit in Australia and New Zealand. In most universities, it is a major consideration for gaining an interview and a seat in medicine. Unlike other requirements, such as good performance in final-year-school or university exams, it’s not necessarily based so much on knowledge as it is on non verbal and verbal problem solving skills and empathy. This is the official site which outlines the exam and basic preparation for them: https://www.ucat.edu.au/ucat-anz/practice-tests/-strategy .
Basically – there are 3 styles of questions. Previously – they were divided into ‘sections.’ You could only do section 1 type questions in the first 60 or so minutes. AFter that time was up, only then could you go onto Section 2 – with everyone else starting that section at the same time.
Now, all these questions are jumbled up.
“Section 1” questions give a passage of writing on a random topic or a logical assumption and then ask you to make logical assertions of it. It could be on anything – and though some of it is medical, most of the time it’s not. Indeed, in some years, they didn’t have ANY medical sections – so don’t feel you have to study biology at all.
Section 2″ questions give passages about a few characters and ask you to make judgements on people’s character, emotions and responses.
And “Section 3” questions test your non-verbal reasoning and give you patterns and ask you to pick the option most likely to be next in the pattern, which one should be in the middle or which one is missing. Think puzzles. The hardest thing about the exam though is arguably the time factor. It’s a 3 hour test but filled with long passages and challenging questions.
This post will not be focused on the best tips to tackle individual questions; there are many programs and blogs designed to help you on that topic, but rather on general tips, exam taking strategy and techniques that will help you in the exam. So here you go. The 7 best tips I give to people who do this test.
In long passages, which come up heaps in section 1 and 2:
1) Read the Questions, before ANYTHING, and PLAN accordingly.
1) – Have a look at the questions before you read the passage so you understand what you need for and then underline bits that will be, or seem important as you go along (so you can refer back to them later on). This is one of the best tips I can give, because it saves you so much time when compared to you effectively having to re-read the whole passage as you look for one or two key points. People say that you should skim read and stuff like that – me – I make sure I understand EVERYTHING that needs to be understood before moving on.
Instead of skimming through and having to reread a passage, 2 or 3 times, it makes more sense to just do it once and do it well.
By reading the questions first – you know what you can skim, and what you need to focus on to understand this.
2) You can’t be perfect. Time is a huge factor! So don’t be worried to skip it!
Don’t be afraid to skip or make educated guesses on questions. The UMAT is time intensive – so once you get a good guess or narrow it down to 1 that seems likely, don’t spend too long worrying about if it’s wrong or right – just move on.
3) Practice previous papers for Section 3 puzzles, and get a grasp of how to answer the main puzzle types!
With section 3 style questions – there’re different questions with patterns. Narrow it down systematically, as you can for most of them, then it becomes easy. For eg – “pick the middle” or “pick
the ‘x’th” ones where they give you 5 options, 3 will have a similar pattern, meaning 1 of those is the end, 1 is the beginning and 1 must be the middle. Narrow it down from there, pick the
most likely of them after that and move on. You can check if they’re right if you have time at the end of the exam.
4) Get some vocabulary down pat for section 2 – and understand them!
For section 2 type questions – know the key vocab vocab. That was my worst, not because I couldn’t empathise with the characters’ feelings and situations, but because for some of them, I just didn’t know what a word like “indignant” or “beatific” really meant haha. So get delectable, despondent, those kinds of words through your head and make sure you understand some of the common words that come up.
5) For the empathy questions – think about WHY they’re asking you these questions.
Think like a doctor would think. Think about WHY they have section 2 style questions. They set questions that try and judge how you respond to the world, and they want doctors who are empathetic, who understand, who aren’t judgmental. Good people see good in others.
So if there’s 2 options which seem similar but one is a more severe, or more evil reaction to a situation, pick the one which makes the persons actions seem somewhat reasonable. So don’t pick “jealous” or “angry” or “contempt” pick “reluctant gratitude”, “despondent” or “disappointed.” unless it really seems like it is just that for the character or subject they’re talking about. For eg if the
question was”how did I feel after the fish came off the line” you wouldn’t say “Pissed the f*#* off” or “angry” you’d say something less severe like “disappointed”. A bit of an extreme example and one that may seem ludicrous (’cause if you know me, you know I get really, REALLY MAD when I miss a fish), but the message is the same.
Those are the major “test taking skills” I used when I sat them. Remember, the tests aren’t the same as when I did them – the “section” style questions are mixed around, but that’s okay – it
means you won’t be as pressured for time and that if you’re good at one section compared to another, you’ll get more time to focus on your weaker styles of questions or more time to go back and
check!
6) Even better than ‘studying’ or doing ‘drills,’ is just to READ
But the best thing I did – I didn’t really do that much practice or that many practice papers – was I read in my spare time. A LOT. And I read widely too. And that made my reading speed, empathy and basic comprehension pretty damn good – perfect for a test like this. Section 1 type questions ask for you to interpret anything from some kind of scientific scrap of knowledge (it usually has nothing to do with medicine), to instructions on how to play table tennis. By reading articles from newspapers, as well as science journals, and indeed – other posts on my blog – you’ll gain speed in comprehension. And learn more. By reading novels, or even better – short stories – you grasp what kind of things section 2 style questions ask.
I’d always be reading a good novel before I slept – it was a habit, I needed to before I slept. On top of that, I read things like TIME magazine, science/technical journals. it’s even easier to do it nowadays, and it’s not a chore at all – a lot of the things you can read are really interesting.
Rig the algorithm, and fill your news feeds with stuff that makes you learn passively. The I Fucking LoveScience Facebook/ Web page is a good place to start – it has a great science blog where it
talks about recent advancements, which are all interesting and fun to read. All of this makes comprehension/ reading speed go up, and also gives random pieces of knowledge to you, which who knows, may just get you more marks. That’s exactly what you want in this kind of test!
I guess those are some of my best tips for the actual UMAT – that’s what I did and ended up doing pretty well, even though I really didn’t prepare for it too well (I was in the 98th percentile, with an overall score of around 200, though I can’t remember exactly).
7) It’s not the be all and end all. Remember that.
But the best tip I can give is a simple one. Don’t stress or panic. I talk about it in detail in this blog post I wrote not too long ago. I talked about stress and how it makes you perform worse… not just for tests like this, but for life in general – and – more importantly – I talked about how to deal with it. Stress, worry and panic won’t help you on the day.
If you go in thinking “OMG this is life or death!”, “what if I forget stuff?” or “I’m not gonna do well!” you doom yourself to panicking, having mini-breakdowns in the test, a confused overworked mind and just feeling bad about yourself, which all lead to you being more likely to fail. If you instead go in on the day thinking “well, I’ve done what I can, all I gotta do is give that damn test” you’ll do yourself a great service. If it’s hard to see that in the day, the best advice I can give is to take a step back and look at the second, more constructive attitude you can take going into the exam.
Instead of thinking about what there is to lose, think about what you have to GAIN.
The chance to make your career one where you spend every day of your life helping others, while doing well for yourself too. THAT’S how you’ll give yourself the best chance of making it.
GOOD LUCK! Feel free to ask for more tips, advice, or your own tips. And feel free to splurge or vent and I’ll try and help you feel better about yourself!
Sign up to my newsletter, and I’ll keep you up to date, and probably send a few sciencey articles that’ll help with your UCAT on the way 😉
But no seriously – if you ever wanna talk – email me at info.at.nikhilautar.com
Effective altruism is a movement that’s revolutionising the
way we give to the poor. Peter Singer described it as “one that combines
both the heart and the head.” The heart empathising with and wanting help
the less well off; the head ensuring our efforts to do so went the furthest. That’s
where the concept of effectiveness comes in. A hundred dollars given to a Guide
Dogs foundation will pay for less than 2 days of training (Guide Dogs Foundation, Australia, 2014); that same hundred dollars
could provide a reliable source of clean water to 300 people in Sierra Leone (World Vision, 2014). That’s not to say guide
dogs aren’t a worthy cause; but individuals, charities, businesses and
governments have begun to realise that the world’s most deprived regions are
where we can cause the greatest change, and that by directing a majority of our
funds there, we’ll create the greatest change.
Peter Singer’s Amazing Ted Talk on the topic of Effective Altruism
But though our heads are starting to temper the way these
funds are directed, it’s the heart that we target to gain those funds in the
first place. And it’s the second concept of the movement, altruism, that describes most of our efforts to help thus far. At
its core, altruism encapsulates the very essence of humanity; our ability to
care for wellbeing of others and the act of putting their interests above our
own is an anomaly of survival of the fittest arguably unique to our species.
But the very words ‘charity’ and ‘aid‘ exude connotations of personal sacrifice,
and the fact that only 5 of 22 OECD countries give the agreed upon 0.7% of GNI
towards Official Developmental Assitance (OECD,
2012), and a 40% drop occurred in private flows to charities from 2007-2008
due to the GFC (World Bank 2009)
shows that that sacrifice, especially in the face of adversity, is often deemed
too much; the reward of a warm, fuzzy feeling too little to justify the
expense.
But what if the rationality of the
mind, which so often gives us excuses not to give, could be used to justify giving
more? What if we viewing charity beyond the strict confines of altruism; what
is we saw charity as a win-win?
Well, in many cases, charity is already just that. Though it
seems counterintuitive at first, there are already many ways governments,
corporations and individuals benefit themselves fiscally, as well as morally,
by helping those less fortunate than themselves.
The rise of the concept of Corporate Social Responsibility
in the 1950s signalled a change in the ideals of businesses as they recognised
their success was intimately entwined with a satisfied, thriving population. Since then, the benefits of engaging in
charitable behaviour on increased productivity and moral capital have become
well documented. Businesses, large and small, that allowed employees days off to
volunteer for instance, saw dramatic increases in workforce morale and
productivity (Smith 1994; Points of Light
Foundation, 2005) and thus concepts such as “volunteering days” or “community leaves” were born. Similarly, larger corporations; particularly those in
disputatious industries, that engaged in strategic corporate philanthropy generated moral capital that mitigated the severity of sanctions and
unfavourable press against the firm when bad acts occurred (Fombrum 1996; Jackson 2007; Godfrey, 2005). This benefit of giving is great, but CSR has to grow beyond just a way of patching up the mistakes companies have made, and with the growing disgruntlement of the wider public to corporate irresponsibility leading to wide backlashes, indeed, they can’t afford not to engage in more generous acts.
But this isn’t a knife to the throat of businesses. Because the benefits
of engaging in corporate philanthropy are wide-ranging and already evident. And they go beyond those of improved
productivity and public relations…
Brand image is of vital importance to a
company’s success, and acts of charity have excelled beyond that of maintain ethical practices and adherence to codes and guidelines; they’ve become a marketing tool. A wide-ranging survey found that 89% of consumers are likely to switch brands similar in price or
quality for such a cause (Cone
Communications 2014). And strategic charitable initiatives taken by
companies, those initiatives in line with their core values, benefit not only the recipients, but
also the companies who organise them. Monsanto partners with many governments
in the third world to reduce world hunger through programs such as Project
Share, which provides farmers in India with education, tools, and their
superior genetically modified seed (Monsanto,
2014). This allows farmers to make the vital jump from sustenance to
commercial farming, gaining them not only free publicity through press
coverage; restoring Monsanto’s widely denigrated image of a greedy, “GMO producing (and therefore evil)” corporation,
but also creating farmers who will go on to become future customers themselves. This is but one example
showing how acts of kindness by businesses often turn out to be wise investments.
Over the years, consumers have become more and more willing to switch brands for companies that give more.
Cause related marketing, and the charity-business partnerships
that are born of it, have proven to increase the effectiveness and impact of
money given by corporations by reducing the reduce the costs of setting up while
also significantly improving brand image, as it associates the brand’s values
with the charity’s own (Porter and Kramer
2002). The Red Revolution, where companies
such as Nikon and Starbux donate 10-50% of profits of product-lines with red labels to the Global AIDS Fund, allow consumers to make an impact
in their day-to-day lives while helping the company sell more product. This movement
is extremely effective, as it reduces the cost required to set up individual programs,
and the benefit to a brand that participates in this program is two-fold. Not
only are they improving brand image, they’re also getting a more
distinguishable, preferred product on the shelf. Positive brand image not only
to increased sales in the short term, but also garners businesses highly desired brand
loyalty. Potential customers are more likely to buy products from companies
that care, not just once, but over and over again (van de Brink et al, 2006; Hsieh A, Li C, 2007). The concept of microfinance,
which achieves staggeringly low default rates of less than 1% consistently (Grameen Bank, 2013; Field and Pande, 2008); a lower risk than a mortgage in the developed world, is further proof that the
gratitude of charity pays off directly. Those who benefit directly from
the company’s aid programs, as well as those in wider society who appreciate
their values, are more likely to be loyal customers of that brand.
The power of the gratitude of those alleviated from poverty
seen in the microfinance industry brings to the fore another, less widely
acknowledged idea. That the alleviation of the burdens of poverty results in
increased consumerism and the development and the growth of emerging markets in addition to better
quality of life. And transnational corporations, particularly those from services
and technology industries, are already benefiting from this growth. The surge
of the middle class in China and India is living proof of this concept. Sony
forecasted a tripling of phone sales in China alone over 1 year [11], and Cisco System’s is
already providing nearly 40million homes in India with our equivalent of cable [12]], and as of 2009, GM sold
more cars in China than it did in the US (Ernst
and Young 2014), highlighting the gains that can be made by pushing more of
the world’s poorest into the middle classes. The benefits to the poor countries are clear and staggering to say the
least; every 10% increase in the number
of people earning between $10-100 a day corresponds to a 0.5% rise in growth (Bhalla 2007), and the number of people
in that bracket is set to double to 3billion by 2030 (Ernst and Young 2014). Imagine how much companies and the world’s
poorest stand to gain by accelerating this growth further, and by establishing themselves and their brands early in the developing world through charity. Though the benefits to bothare clear, it can
be argued that the profits from human development take time and great
investment to be realised. But even now, the world’s poorest are holding
markets that corporations and businesses are targeting. Microsoft researchers published
a paper on how to increase the efficacy of mobile phone sales in Mumbai’s slums (Rangaswamy & Nair, 2010), showing even
the world’s least-well-off are beginning to access technology. Taking away their
biggest obstacles; basic sanitation, employment, housing and attainment of
education, is not only the cheapest, most effective way to help them; it’s also helping us too.
(cone communications 2014)
Governments are in a unique position of having both the political
and financial power that charities and businesses lack, which is why they’re
responsible for 80-85% of developmental aid that breaks down these barriers (OECD, 2014). Developed nations’
governments and their people tend to own and dominate the technology, research
and services sectors which stand to gain the most from the development of the
world’s poorest. Thus, despite popular opinion otherwise, it is indeed in their
best interests to foster this development. The bypassing of pharmaceutical patents
by many developing countries which represents a loss of nearly 3 billion
potential customers is
a perfect example of the hazards of the festering global inequality. Yet the
aid budgets of many countries in the Development Assistance Committee have
decreased, as lower than expected economic growth during periods of austerity
calling for the reduction of “unnecessary spending” (OECD, 2012).
It could be argued though that the growth of markets are
long term, non specific benefits of aid, and that governments who give too much
at their citizens’ expense are irresponsible. But official developmental
assistance (ODA) already shows palpable benefits to nations in the short term. Multilateral
aid in particular cuts down the likelihood of international conflicts and
provides a very effective, collaborative way of dealing with crisis situations.
But bilateral aid, which comprises the 70% of ODA (OECD 2014), often directly benefits the giving nation through the
concept of aid-in-kind. Tied-aid programs,
which attach assistance to the fulfilment of certain trade or policy
concessions, are often criticised for being less effective, predatory as
they’re designed to mainly generate income for the donating nation, or for addressing
human rights violations while ignoring the larger issue of global poverty (GAO 2009; Younas, 2008; Pfutze T, 2008;
Younas, 2008). But this trend is changing, with developed countries increasingly utilising the cheap labour and locally-sourced,
cheaper goods of developing nations while providing what them with what they don’t
have; technology and expertise. Australia’s contribution to the Small Hydro
power Scheme in Remote Fijian villages is a perfect example of this. Villagers were
allowed access to electricity for the first time, gaining them the ability to
store food and for children to study at night, while hydro-electric companies
and engineers from Australia gained contracts, stimulating economic activity in
Australia’s while also gaining the nation valuable expertise (Liu et al, 2013). And indeed, the very
engineers who participated in that program went on to help design the Snowy Mountain
Hydroelectric Scheme, which provides Australia’s largest state with 10% of its
electricity usage and invaluable irrigation to this day.
But if charity is already such a no-brainer; why isn’t more
of it happening? How do we make the benefits clearer, in order to get it happening more?
The lack of evidence for the benefits of giving is part of the
answer. Though there are numerous
studies linking Corporate Social Responsibility to improved financial performance
(Margolis and Waslh 2001; Griffin and
Mahon, 1997) , little evidence exists quantifying those benefits (Vaidyanthan, 2008). Some suggest the
lack of consistent theory behind the benefits of giving are to blame (Margolis and Walsh 2003; Smith 1994), others that the methodology and sample sizes aren’t
consistent or reliable enough (Griffin and
Mahon 1997; Porter and Kramer, 2006). But whatever the reason, it’s impossible
to justify charity as an investment to
shareholders and voters when you can’t put a dollar figure to it. Securing this
data will cause change, but it’s only part of the answer. The development and
emergence of markets due to human development, the concept of customer and
recipient loyalty leading to profits, the improvement of brand image and international
relationships can’t, or aren’t even being measured as benefits of giving to
this day. Thus, a paradigm shift, along with increased investment, into how we
view and study aid is required to get reliable data on the benefits of giving.
This data will make giving something businesses and governments can’t afford
NOT to do.
Perhaps people simply aren’t aware that giving can be mutually
beneficial. The semantics of giving and the sacrifice it’s associated with are
in part to blame for this, but lack of awareness of both the efforts companies already go
to for others, and the society-wide benefits of giving are part of it too. The
Red Revolution discussed previously is backed by large corporations such as Coca-Cola,
Starbucks and Apple; yet most reading this wouldn’t have even know it existed. I
know I hadn’t before I wrote this. If companies were to actively advertise
their efforts to help others more, not only would they benefit themselves through
increased sales and business (and put the onus on others to match them, thus
causing a chain effect that will increase the private sector’s contribution to charitable
causes), they’d also achieve another goal. Making the public aware that giving
can be a win-win. Charities are beginning to realise this too and are opening the eyes of the public to the idea that charity
needn’t be something that comes at their expense through giving people more interactive, more fun
ways of giving. TheUNICEF-Tap-App,
in partnership with Georgio Armani, is a perfect example of this. The app is helping thousands kick their smart-phone
addictions for the wonders of real life by giving them compelling motivation to
do so; the donation of a day’s worth of water for every 10 minutes users spent
off their phone. Smaller organisations, such as the Louis26 Foundation,
dedicated to helping cancer patients and their families through tough times,
organise parties, get-togethers and sporting events, with all proceeds going to charity, allowing people to enjoy
some respite from their daily lives without the guilt of self-indulgence (Louis Segregato 26 Foundation, 2014). MaterHomes runs lotteries with statistically
higher chances of winning per dollar spent; satisfying both the innate fascination
and desire of a decadent, luxurious life and the more accomplishable,
gratifying goal of helping others simultaneously. And microfinance
organisations, such as Kiva, are increasingly allowing users the option to
withdraw money if they wish to attracting not only altruistic donors, but also
those looking for a reliable way to save.
(Click on any of the above to do these – I’ve personally participated in all of them – and they get the satisfaction of helping others without ever having to go out of my way or hurt myself financially for doing so.)
It could be argued that this mentality of benefiting yourself
while helping others corrupts the very
ideals of giving. That it would create a business minded approach to charity
that would compromise that which we already gave to the more needy. But that allegation
assumes that people currently give only to gratify themselves, or because society
deems that they should. The heart is the core of altruism. And our compassion,
and willingness to help others will not diminish as long as inequality exists
in this world. The power of humanity will not be smothered by perceiving
charity as a win-win; it will be unleashed, as it unfetters the concept from the
chains of sacrifice that binds it. If people were to realise that charity is a win-win,
then people and the governments and businesses which exist to serve them would
be more able and willing to help others. Something that all humans are programmed to do,
deep inside. If businesses and governments, who control and regulate the entire world’s resources finally came to the realisation that the developing world has the most people, and stands to be the largest markets in the future; if they finally saw that they’d secure their prosperity by investing in, rather than holding back their potential, then charity wouldn’t just be a great investment, but one they can’t afford NOT to do.If we could expand the scope of global development from the spare change in ones’ pocket to the entire bank’s own interests, if we could bring the $100trillion world economy to realise that growth need not come from the subjugation of others but rather the advancement of us all… we will finally cure poverty.
This was a longer version of an essay competition entry I wrote for Bill Gates. Have a read of it and tell me what you think! Also let me know any other ways you can benefit yourself by giving to charity (I’ll be expanding on this and adding chunks to it over time, and showing more ways of how you can benefit by giving to others – and I’ll give you a mention for any idea I add in there!) Also – let me know what you think!
References:
[1] Singer P, (2013, May) The Why and How of Effective Altruism, Retrieved from: https://www.ted.com/talks/peter_singer_the_why_and_how_of_effective_altruism
[4] World Bank
(2004), World Development Report 2005: A Better
Investment Climate for Everyone, World Bank, Oxford
University Press
[5] World Bank
(2009), Global Development Finance 2009: Charting a Global Recovery, Global Development
Prospects 2009
[6] Smith, C. 1994.“The New Corporate
Philanthropy.” Harvard Business Review
[7] Points of Light Foundation and the Center for
Corporate Citizenship at Boston College. 2005. “Measuring Employee Volunteer Programs:
The Human Resources Model. “
[8] P. Godfrey, “The Relationship between Corporate
Philanthropy and Shareholder Wealth: A Risk Management Perspective.” Academy of Management
Review 30(4):777-798.
[9] C. Fombrun. Reputation:
Realizing Value from the Corporate Image.Harvard Business School Press 1996
[10]K. Jackson, “Building Reputational Capital: Strategies
for Integrity and Fair Play that Improve the Bottom Line. New York: Oxford University Press, 2004
[12] Hsieh A, Li C, 2007, “The moderating Effect of
Brand Image on Public Relations, Perception and Customer Loyalty”, Marketing Intelligence and Planning, Vol 26
Issue 1, 26-42, 2008
[13] Brink D, Schroder G, Pauwels P 2006, “The Effect of Strategic and Tactical
Cause-Related Marketing on Consumers’ Brand Loyalty”Journal of Consumer Marketing Issue 23/1
(2006), 15 – 25
[12] Porter, M. and Kramer, M. 2002. “The Competitive Advantage of Corporate Philanthropy.” Harvard Business
Review 80(12):57-68.
[13] Field E. Pande R 2008,“Repayment Frequency and Default in Micro-Finance: Evidence
from India”, Journal of the European Economic Association 6,
501.509
[14] Osnos P 1998, “TheEconomist
Microlending From tiny acorns”, Grameen Bank 2013, Retrieved from: http://www.grameen-info.org/index.php?option=com_content&task=view&id=215&Itemid=541&limit=1&limitstart=9
[15] Pakistan Tehreek-e-Insaf 2014, Cisco’s
solutions now reach over 40 million homes in India, Economic Times May 2014, Retrieved
from:
http://economictimes.indiatimes.com/articleshow/35722108.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst
[16] Bhalla S 2007, ‘Second Among Equals: The Middle Class Kingdoms of India and China” Comparative Economic Studies 09/2011; 53(3):355-381.
[16] N Rangaswamy, S Nair, “The
Mobile Phone Store Ecology in a Mumbai Slum Community: Hybrid Networks for
Enterprise” Information
Technologies and Development Journal, Vol 6, Issue 3 –
Fall 2010, 51-65
[17] OECD (2014), “Development aid: Net official development
assistance (ODA)“,Development: Key Tables from
OECD, OECD 2014, No. 1.
[18] OECD
press release, Development: Aid to
developing countries falls because of global recession, OECD 2011,
retrieved from
http://www.oecd.org/newsroom/developmentaidtodevelopingcountriesfallsbecauseofglobalrecession.htm
[19] United States, Government
Accountability Office, “INTERNATIONAL
FOOD ASSISTANCE; Local and Regional Procurement Can Enhance the Efficiency of
U.S. Food Aid, but Challenges May Constrain Its Implementation,“ GAO-09-570 International Food Assistance, May 2009
[20]Younas, J (2008) “Motivation for Bilateral Aid Allocation:
Altruism or Trade Benefits”European Journal of
Political Economy, Vol 24, Issue 3 – September, 2008, 661 – 674
[21] Easterly W, Pfutze T, (2008) “Where
does the money go? Best and Worst Practices in Foreign Aid” Brookings
Global Economy and Development, June 2008
[22] Liu, H., Masera, D. and
Esser, L., eds. (2013). World Small Hydropower Development Report 2013. United
Nations Industrial Development Organization; International Center on Small
Hydro Power
[23] B Vaidyanathan (2008),
“Corporate Giving; A Literature
Review,” Center for the Study of Religion And Society,
University of Notre Dam, October
2008
[24] Margolis, J and J. Walsh,
(2001) “People and profits? The
search for a link between a company’s social and financial performance.” Mahwah, NJ: Erlbaum.
[25] Griffin, J. J. and J. F. Mahon, (1997) “The
Corporate Social Performance and Corporate Financial Performance Debate:
Twenty-five Years of Incomparable Research.”Business and Society 36,
5–31.
[26] M. Porter, M. Kramer, (2006) “Strategy and Society; The Link Between
Competative Advantage and Corporate Social Responsibility” Harvard Business Review, December Issue 76
– 94
[27] Margolis, J. and J. Walsh, (2003).
“Misery Loves Companies: Rethinking
Social Initiatives by Business.” Administrative
Sciences Quarterly 48: 268-305.
[28] Louis Segreto 26 Foundation
2014, Retrievable from: https://www.facebook.com/ls26foundation/info
Recently on Facebook, a few pages dedicated to cancer awareness asked patients to describe themselves and how they feel in one word.
Here’s an example.
I liked how positive people’s responses were. I like how these pages are getting groups of people in tough times together. I loved the word “Surthriver”.
But there’s one that stands out to me. The one with no likes.
“.. Invisible.“
People always tell me I’m brave for being so happy and positive through my journey. They admire how I’ve adapted, and grown, through my experience, and I give off that impression of a “surthriver” on my posts, I’m sure.
But the ugly, not-too-well-known truth about cancer is it’s not something that you have for a while that either kills you or spits you out to keep going.
Cancer affects you long after its left your body… the physical fatigue, maintenance treatments and weariness is just the tip of the iceberg. The emotional drainage of facing your mortality, sometimes multiple times, the frustration of an all-too-slow recovery and the realisation that you may never be your old self again plagues many cancer patients long after their last treatment is over. Not to mention the medical bills…
But surviving cancer is still hailed as a victory. Something to be celebrated.
And cancer survivors, survivors of any tragedy for that matter, are hailed as heroes – symbols of strength – physical embodiments of those words badass, brave and blessed thrown about in that Facebook post above.
It’s gotten to a point that survivors are expected to be act that way….
Well, that expectation is UNFAIR.
And it’s leading to many survivors hiding their true feelings, not talking about it and not getting help.
It’s leading to many feeling ashamed or weak when they don’t feel the same way.
And it’s leading to people getting depressed when they realise that cancer affects you long after treatment stops…
Telling someone, or expecting them to feel glad that they survived cancer is like telling war veterans with PTSD that they should be glad they’re alive…
It’s not easy being grateful for the worst thing that’s ever happened to you…
And the pressure we, as a society, put on these survivors to feel that way is not helping.
How we’re expected to act and behave, despite how we feel
SUCKS.
And if you feel the same way .. or if you, or a loved one are wondering why you’re not in that constant state of euphoria everyone talks about for beating cancer, believe me –
YOU’RE NOT ALONE.
I come off as happy, positive, cheery even in the fact of adversity. As someone who’s adapted well to this journey. Someone who’s won their battle.
I don’t feel like I’ve won…
I hate that I got cancer. I hated having to suffer through it.
And to this day I still suffer because of it. I spend more
time at the hospital getting treatment and waiting around for appointments than I do at university or hanging out with friends.
I get aches, spasms and cramps every day for no apparent reason. I have skin
peeling from my body, that itches incessantly and I can’t do anything about it. I get tired for no reason, I
fall in and out of depressive moods week by week and I’ve had to go from not
being able to walk for all the tiredness to being able to live a normal life 8 times now.
It’s been 3 LONG years…
and I’m STILL not done with this!
I don’t feel
like blessed… I don’t feel brave… I don’t feel proud…
I don’t feel “glad to be alive”… not all the time.
I’m not alone here either. In fact, I’m representing the majority of survivors here. This reflection by another cancer patient on the untrue, frustrating stereotype that cancer survivors are expected to encapsulate, went viral and had huge support. 56% of cancer patients seek some form of psychological or medical emotional assistance in their treatment. Remember – not everyone is open, or can get access to that help. I’m sure everyone with cancer needs it, at some point in their treatment.
Even those survivors, like me, who come off as mostly happy and positive don’t feel that way all the time.
It seems absurd that I have to say this. But it’s perfectly normal to feel bad after cancer…
You don’t have to put up a facade, or berate yourself for the expectations of others.
And it’s okay to feel down and pissed off every now and then. Everyone does.
And you’re not weak to admit that you’re going through pain and suffering, physically and emotionally. In fact, it’s pretty brave to admit that you are.
But it shouldn’t have to be that way. You shouldn’t be ashamed that you’re finding things hard.
I’m writing this to let you know that you don’t have to be brave, badass or blessed to beat cancer. You don’t have to be those things to get through periods of depression or hardship or to accomplish anything in life for that matter… this part of my message applies to anyone.
How would I describe myself in 1 word?
The way I’d handled all of this, how I’ve adapted and changed after cancer… I’d have to say that I was
“smart.”
The words I took to heart most when I was diagnosed weren’t those cliched “You’re strong!” “You’re brave!” or “You’re a fighter!”…
And also the the words of a nurse who told me, the day after being diagnosed that the next few weeks would be filled with pain, nausea, diarrhea, fevers and tears.
I didn’t go into my battle kidding myself. I knew it would be a long haul.
But I realised, when I took a step back and thought about it, that the fact that I knew and could acknowledge the pain that was coming meant that in the future, I wouldn’t give up when that pain got real. That I’d be prepared for it. That I would look at what would come after hardship rather than linger on it.
Realising and accepting that I was human, that there were things I couldn’t control, that it would take time to get better didn’t bring me down into despair… In truth it left me only one way to go. Up.
It was what allowed me to take a step back and look at where I was, without any delusions of grandeur or expectations of miracles. And that allowed me to see where I was and what I what I should do going forward with a startling clear logic.
Accepting that there were hard times to come, acknowleding that I was scared and worried made me focus on how I could get past my issues. And taking a step back and realising that only I could make myself feel down (no-one comes into your head and programs emotions into you – only you can) made me see that I actually had a choice on how I viewed my life and my journey. From there… choosing to have an attitude and living life on the path that made me happiest and healthiest became the only smart thing to do…
Looking in the big picture, and focusing on what I could control rather than what I couldn’t was what got me through this. NOT some inner strength or positivity or the blessing of others (though they were always appreciated).
That’s something ANYONE can do. It’s not as hard as you think.
In fact – taking a step back and looking at where you are objectively, then acknowledging the hardships and doubts you have and planning your way around them will help you see a second, healthier and happier way of looking at life. And once you do that, choosing to view and live life on that path will be the easy, logical choice.
You’re not WEAK if you think life is hard and painful sometimes. You’re definitely not ALONE.
In fact, You’re NORMAL.
You don’t have to be strong to get through strife. Strength, motivation and the blessings of others help…
But the best thing on your side in your battle is YOU.
And I hope this can help you get you on your side.
For those who know others are going through hard times , whether they be cancer survivors or not I hope this lets you know that just because they seem to be coping with it well – doesn’t mean they are. That simple question, “Are you okay” saves lives.
Stopping that unfair expectation and breaking that stereotype of a survivor starts with YOU.
This was a reaction to this post – one of the most awesome reactions to a post of mine ever.
And this was a talk I gave on this issue not too long ago:
Another place where this post was shared and the reactions, the almost coming out of other survivors after reading this is amazing. You’re not alone.
“Survivors are too often expected to put on a happy face because the cancer is “finished”. But that expectation is…
Posted by I Had Cancer on Friday, 23 October 2015
As usual – if you ever wanna talk, about anything I’m here.
The other day, I was out to dinner and drinks with some friends. Amidst our casual banter about work, life and play we somehow got onto the topic of depression. It’s something that’s affected my friends, family and myself over my 3 years of being a patient.
One of my friends said something that got to me.
“Being told you’re depressed gives you an excuse to not try to get better. Maybe if people who say they’re depressed tried more, they wouldn’t be depressed.”
He didn’t mean to be judgmental or mean about it, in fact, he was sincerely concerned for their welfare.
But it was obvious that he didn’t know what depression does to you. That it saps away at your energy, your very ability to feel happiness, to the point where you don’t even want to get out of bed.
Someone else brought up a relative who’d been through depression and agreed with him whole heartedly.
I tried to tell him about how depression really affects you, and talked about how I got out of it (by taking a step back, questioning what I was doing and eventually, seeing another way of looking at things, and talking to people about it). But he still maintained this idea that a majority of people use their depression as an excuse to not try – that it’s their fault they’re depressed.
When we look at ourselves, we’ve programmed ourselves to look at the bad rather than the good.
We label ourselves every day.
And it doesn’t just apply to issues like depression either…
We tell ourselves we’re not smart enough, not good enough, not cool enough to do what we wanna do. To get into our dream course, our dream job, to try out for the
first grade team or to ask that girl you like out on a date – we always use how we label ourselves as an excuse to not try.
These labels are garnered by how we grew up, how we were raised and by what we believe other people think of us.
But when we say that we’re either smart or dumb, or that we’re weak or strong or that we’re hot or not, it’s not always a bad thing.
These labels can be useful.
They allow people who are depressed or going through hard times to cut themselves some slack, and allow them to ACCEPT what’s happening to them.
And a lot of people look at themselves, and use those labels, either self-imposed or not, to improve themselves.
But it’s when we start to BELIEVEthose labels, when we let themDEFINEus that they stop ourselves from trying to get better.
If you’re someone who has gone through trauma, or depression, however, it’s only a natural reaction. You shouldn’t feel bad for feeling crappy about the worst thing that’s happened to you. It’s normal.
But sustaining this feeling, and using our disabilities as an excuse, only leads to us harming ourselves in the long run.
Half the time though, we don’t even know we’re labeling ourselves.
After thinking about his words, I took a step back and had a look at what I was doing, about 10 months after my transplant.
I thought about where I was at objectively, without any bias, and realised that despite not having any major treatments, despite not being hospitalised in a while, I still thought of myself as a patient.
That wasn’t a terrible thing – acknowledging my vulnerability would make me cautious. I’d watch what I ate, ensure I’d take extra care in terms of hygiene, sanitation, that I’d stay away from sick people and all the other things I needed to do to stay healthy because I knew I wasn’t a patient.
But I realised that at the same time I WAS USING IT AS AN EXCUSE to not
get fit, not want to learn, to not eat healthily, to sit around and be a slob.
It was stopping me from getting better!
That dinner was 2 months ago.
Since then, I’ve resolved to improve myself. Slowly, over time, I kept reaffirming and telling myself to not label myself, to not use my cancer as an excuse, in my head.
I did it slowly, by first doing little things that I was telling myself I couldn’t, or shouldn’t be doing, and then building up until I could do them.
And slowly, but surely, that became a habit… Your brain’s neuroplasticity and the power of affirmation and reinforcement, ensures that you can change your mindset on anything. Even if you feel like you can’t today (I’m a medical student, and researcher. Check out my book that I’m writing for the science behind this, and my own story!)
And today I’m proud to say that I don’t believe that I’m a patient
anymore.
I don’t see myself as a depression sufferer either.
I see the value of being cautious. It ensures I have motivation to stay
healthy, it allows me some leeway to take breaks when I need them, it ensures that I won’t push my body too hard in my quest to regain my health. It ensures that I’ll always ask for help if I need it, when I’m down. I see the benefit of that label.
But I’m not going to use my “being a patient” as an excuse to not push forward now. I’m no longer going to take a day off because I may have felt dizzy a few days ago, no longer not go on a run because my legs are too sore, no longer going to stop myself from going to classes because I shouldn’t be around too many people UNLESS I REALLY HAVE TO.
I’m not going to lie to myself anymore.
It wasn’t easy at first. But a change of place, a change of atmosphere, A CHANGE IN ATTITUDE really helped me get there. I started by going on a daily walk up and down a long hill, doing little bodyweight exercises like sit-ups and push-ups and helping out around the house. And I slowly built up from there.
I knew that I wouldn’t see results straight away, that I’d feel tired at times, and lazy at others. But I’d push through those times. Eat well, at the right times to make sure that I didn’t even feel that lazy feeling.
I knew that at times, I’d have to take breaks, especially when I’d be getting my treatments.
But I reminded myself that I wouldn’t use my sickness as an excuse to not try.
I’m glad to say it’s working.
Because of my consistent work, because of my commitment to getting healthier and because of me not using my past as an excuse, I‘m happier, healthier and fitter than I have been since being diagnosed.
I’m running around, I’m going to classes, I’m playing basketball and I’m looking and feeling better than ever, since finding out that I had cancer.
I’ve been a patient now for nearly 3 years.
Today, 1 year after my 2nd Bone Marrow Transplant I no longer think of myself as one.
And to those of you reading this – I hope this inspires you to stop using these labels as an excuse too.
Have a look at yourself, and see what you label yourself as.
If you find yourself telling yourself you’re too sad, stupid depressed or weak to do what you want, do exactly what I did.
Take a step back, have a look at yourself and question why those labels DEFINE YOU.
And once you do that – take your time, take little baby steps and you’ll
STOP YOURSELF
FROM STOPPING YOU.
If you think you’re not smart enough or accomplished enough to do something, ask yourself why?
No-one was born with the ability to read, to do calculus, to do propose theorems. THEY MADE THEMSELVES PEOPLE WHO COULD.
If you wanna get that job, get into that course, pass that paper –> try your hardest, work smart, not hard and you can get to where you wanna go. It won’t happen straight away, but if you work hard, ask the right people for help and work your way up like I did, you give yourself the best chance of doing it, don’t you?
If you think you’re weak, or dependent, or just unable to change, take a step back, have a look at yourself and you’ll realise that just telling yourself that is stopping you from trying. Instead, take small steps to improve yourself. Give it time – weeks, maybe months, and you can change yourself to become the happiest, strongest version of yourself.
If you think you’re depressed, and bound to stay that way, maybe, just maybe, you’re making yourself more likely to be that way too. When you next are in a good mood, when you’re feeling happy and able to do this; set up a system of talking to others, whether it be friends, family, a professional psychologist, and you’ll give yourself the best chance of getting better. You may have had some bad things happen to you in the past, you may have grown up to be that way, you may even have some chemical imbalances that predispose you to feeling that way –> But it’s only you – your perception of yourself which stops you from trying.
Depression isn’t something you have to suffer from forever. It’s almost comforting to be depressed. It becomes your norm. Trying to fight it, to do things seems like way too much effort at the time, so many don’t try to get better.
But in truth – it not only confines us to this box, to us feeling worse about everything… It also isn’t too hard to break out of either. The toughest thing about depression is that it makes us believe that we can’t do anything. But just like teaching yourself how to get past those labels, your brain can be rewired to release more dopamine and serotonin – our happiness neurotransmitters – as your norm. It’s actually easy to do. It just takes time, and a bit of planning. Accepting that it may not happen right away and that you will occasionally fall back into downward spirals every now and then, only allows you to get back up and continue on your trajectory of becoming a happier version of yourself, when you can. Again, this isn’t just conjecture. Neurobiology, and decades of psychological research guide what I say, and the advice I give (again, I’m writing about it – be sure to check out nikhilautar.com/mybooks for more info!).
But yeah. Feel free to contact me if you need help with these issues. I’ve talked to hundreds of people, and not all patients as some of my posts may make you believe. (contact me via here anonymously, at [email protected] or via my FaceBook page)
These labels keep you grounded, they keep you realistic and they can motivate you.
But if you believe them, they only pull you down.
If you give it time, you CAN become the best version of yourself.
And as I said before, if you need any help in your journey, feel free to contact me.
Bree and her friend Bridgette were
diagnosed with leukemia, on the same day, at the same hospital. They underwent
painful, grueling treatment together. They spent the hardest
times of their young lives with each-other…
And now that Bridgette’s died, Bree can’t imagine living without her…
It speak volumes on our ability to love… And how love’s power can even outweigh our ingrained instinct to endure.
It’s
tragic…
But this kind of loss happens every day. And not just to cancer patients like her and I.
I felt a loss similar to hers not too long ago. The loss of my first patient.
To be fair, I’m not a doctor, yet. After my experiences as a cancer patient though, my drive to wanna become a doctor – a dream of mine from childhood – only grew stronger. Hugely. But on occasion, I meet people, either through this blog, from a friend, or at hospital, who are going through hard times. Through my experiences, I try and help them by giving them encouragement, someone to talk to, and, in the case of other cancer patients, who, I guess, make up the majority of people I talk to, trying to inform them of what’s to come (all the
while trying to get them to be happy, despite what could be a long, hard battle).
Before my first bone transplant, I found that having the words of someone who’s been through the process more powerful than those of my doctors. They just stuck, there was just more power and credibility to the words that came out of a fellow patients’ mouth. And about midway through last year, I met a patient who was about to undergo a BMT. He’d been going strong for years after his lymphoma was in remission, but it had come back, and this was his last option.
A nurse responsible for coordinating the transplant asked if I could tell him about the procedure. I started talking to him and giving him tips for the procedure. I comforted, consoled and encouraged him when he got scared.I even prayed with his crying family at one point… and continued doing that through the whole transplant procedure, where I could.
I can still remember
his eyes on the eve of his discharge from hospital.
I’d told him of all the things he had to look out for after the transplant – the possible fevers, rashes, diarrhoea and fatigue, amongst other things. I gave him tips on the recovery process, and assured him that he could do it.
I still remember the laughter of him and his family as I left his room.
Despite his shaking, despite his pain, despite the suffering, his eyes were filled with hope for the future.
Hope that he could, and almost would be normal again.
That was
the last time I saw him…
He died a few weeks later.
He wasn’t old – he was in his 20s, only a few years older than me.
He’d only started living.
HE HAD A SMALL CHILD GODDAMNIT!
When I found out, I was shocked. He was suffering, he wasn’t done with treatments yet. I knew that and he knew that too. But he’d seemed so positive, so sure he’d make it, and the doctors thought so too… but he didn’t.
After that shock, I started asking myself unanswerable questions.
What had he done to deserve
this?
What would happen to his baby?
Why him and not me?
I was feeling the same thing Bree had after Bridgette died… the pain of sheer and utter loss… the pain of losing someone so close to me.
The next few weeks, I couldn’t bring myself to do anything. I didn’t wanna read, write, talk to people. All I did, day in and day out was browse pointlessly through the internet, not even registering what I was doing…
It was only later on that I realised,
that I was told, that I was going through depression.
Frank’s death was a major cause of it, but the frustration of the ongoing treatment and the medications I was on, all contributed to my feeling down… out… and empty.
I could see that something was wrong… I didn’t want it to stay that way.
But it was JUST SO
HARD to even break the pattern of doing nothing and not caring.
Especially after the world
seemed so meaningless, so unfair, after all this.
After a while… when I could bring myself to do it I sat down and asked myself, what next?
It was then that I remembered my own blog post about depression. I looked over that post again. And I took my own advice.
I talked
to somebody about it.
That somebody, for me, was Dad.
I told him how I was feeling, and he listened. He didn’t know about Frank’s death, didn’t know about the loss I was going through. But he gave me another perspective of looking at things… and that would mean the world to me.
Me, I was trying my best to help people. And that’s not a bad thing to want to do.
But he made me see that I was overdoing it – I was giving up my own happiness, sleep and even food only months after my second transplant, a critical stage of my health.
I was staying up late, talking people through their problems, writing too much too often and pushing myself harder than I should’ve been.
He assured me that I would help more people in the long run through my being a doctor, if I first helped myself. I agreed. He also convinced me that I’d help others in the short term if I did that too. I couldn’t write or study medicine if I was stuck in hospital for the next few years, right?
And that helped me see that I couldn’t hurt myself anymore over Frank’s death.
A different perspective was all it
took…
But the question still
remained. How could I get over the loss?
After a while of soul searching, I saw it was exactly what that poor girl was going through. Survivor’s Guilt.
The feeling of regret after you lose a loved one. It’s the same regret when you fail at something at life. Regret that you hadn’t done enough, hadn’t been there enough. It only adds to the melancholy that is loss.
But why was I punishing myself that way, instead of asking what Frank would have wanted for me?
In the end… I knew that he would want
me to be happy. To do him proud.
Why
shouldn’t I do that instead?
Why was I blaming myself for
Frank’s death.
I thought I’d given him hope.
And then stolen it from him…
That was what was eating me.
On top of the loss of a good
friend.
But after a while of asking myself why again, I realised that I had told him of all the risks, of all the pain that comes during and after a bone marrow transplant. I told him he wasn’t done yet – that the recovery process takes years for some.
All I’d done was give him advice for getting through the procedure and speeding up his rehabilitation. And someone to talk to. Someone to visit him, laugh with him – someone to give his brothers and wife a shoulder to lean on when they needed it.
Yeah, he died young, and yeah the last few weeks were filled with struggle. But there was no way I could have stopped that. He’d been unlucky to even get the disease in the first place, yet alone get one the chemo and a transplant couldn’t fix.
That reminded me of a quote
from M.A.S.H.
“Rule
number 1 of war [or medicine, or life], young men die. Rule
number 2, doctors [, no-one] can’t change rule number 1.”
What I’d done was give him some happy moments in the last days of his life. I’d done all I could do. I had made a difference.
That guilt I was feeling was only harming me. Something Frank would never have wanted for me. And realising that allowed me to let that pain go…
But I didn’t want it to end that way.
The loss of this still stuck. The feeling that this was all unfair was still there… But… sad as that was, I couldn’t change that… So… why was I only focusing on that?
The best way I could honour his life, and let him live on, past his time, I realized, was to learn from my experience with him and help others get through what I went through.
That’s what this post is about.
SO WHAT DID FRANK TEACH ME?
· He reminded me that no-one can live
forever, that no-one always wins in life.
· That when we lose someone or
something we care about, we will miss them.
But once we get past our grief and failure, we have a choice on how we deal with it.
· That his personality. His spirit. His impact on this world… Still lived on, beyond
past his time, by how he’d changed those around him. By how his amazing family
gathered around to help each-other. By how he could laugh in the face of much
pain…
· That we can either dwell on the past
and close ourselves off to others and to opportunities…
Or we can learn from them, from the
mistakes we’ve made on our journey with someone or to something, and use that
to not only get over our loss, but also to improve
ourselves.
That way we can be more successful, influential and HAPPY human beings.
Ones our loved ones would be proud of.
It won’t happen in a day. We may have to do some soul searching to get there. When you lose someone close… it’s impossible to ‘just move on.’
If we can’t see any other way of looking at it, talk to somebody about it.
I hope my experience with Frank can help you see your way around your losses.
When you lose someone close to you – a friend, a family member, your mother, your father, your son – you will feel loss, and you will feel pain.
Frank was a close friend. He’ll always be a part of me. I can only imagine how hard it would be to lose a brother, partner or child to this disease…
But after a while, YOU have the choice on how to remember them. So LEARN from those you’ve lost. Let their time on this Earth, let their qualities, their words, their philosophies, or their tragedy, inspire you to be a better person.
They live through you if they’ve taught you how to live.
They smile on as you smile and make them proud.
Always remember that.
****
So What does that mean for me as a med student?
I’ve learnt that I can’t save everyone… I’m only human… people live and die, and no doctor or scientist, can change that.
I’ve learnt that I need to take care of myself before I can help others. I need to make sure I get better first, that I don’t overstress myself (especially now, while I’m still
recovering) and when I become a doctor, that I don’t blame myself for deaths or misfortune I could not prevent.
But does that mean that I, like many doctors, close myself off to others and never get close to patients?
NO.
I’m not a person who can or wants to do that… And I’m not going to turn to alcohol, or other drugs, to get over the sadness my profession entails either. Alcohol abuse is surprisingly high
amongst doctors, despite their better knowledge, for a reason…
What I will do is remember this story, and remember what I’ve learnt from it.
I will still care for others, I
will still connect with my patients, I will ALWAYS try my best to help them in
their times of need.
But when I lose someone, when I miss out on a promotion or fail and exam, when I just feel down and out… I
will talk to someone.
And I WILL
move on.
A talk I gave, on this issue and on the horrible stereotype and expectation cancer patients are expected to live by (read about that here:)
If you or a loved one is facing loss or depression of any kind, you will move past it. It won’t
happen straight away, it will take time. But talk to someone about it, and ask yourself what they would want for you – I guarantee it would be for you to keep being you.
I hope this helps some of you out there who may be struggling.
Or feel free to talk to me, here or on my blog (nikhilautar.com) or on Facebook – wherever. I will try my hardest to help you.
Comment below anonymously if you’d like.
And by the way, Frank
isn’t actually my friend’s name. It’s just a name I made up to protect his, and
his family’s, confidentiality.
Last post:My Story:Next One: Anti-vaccination groups have pushed a scare campaign on the public for years now, claiming that vaccines harm, not help kids.
But the truth is, this whole scare campaign really caught fire, after a literally fraudulent, made up paper, was published years ago. This video explains it well. Check it out.
Anti-vaccination movements have been around for a while, but this whole idea that vaccinations cause autism really started in 1998, after a paper was released looking at only 8 kids who’d ‘developed autism after having the measles vaccination’. But the fact was, that 8/12 of those kids had another disease at the time. Subjects were hired by an anti-vaccination group. Data was completely falsified – in fact NO children were found to even HAVE AUTISM in the study – yet alone 8/12. Since then. multiple studies, ranging from 5,000 to as many as 5 MILLION kids – have shown no association between the MMR (or any other) vaccine and autism. Hell – anti-vaxers even funded a $250,000 study to prove, once and for all, whether this was the case – and lo and behold… THEY FOUND THAT VACCINES DON’T CAUSE AUTISM!
The article was retracted by the journal that published it. 11/12 of the original authors have retracted their statement – something never seen in medical articles before. Only 1, the person who wrote the initial article, a person who makes millions off this campaign, a person who had his medical licence revoked prior to this article being written, still backs his claim.
1) Anti-vax campaigns and groups, though they may have arisen from actual concern, are now powerful. They keep providing funding to enhance their agenda, making people think those who support them are doing good, when in truth they’re unknowingly being led by people who know this information to KILL thousands of dollars a year. Now they, either by accident or, more likely, purposefully, have created a whole conspiracy theory around the idea that the government is trying to cover something up or make people sick on purpose. They invest millions into this and are making millions off it too… while 30,000 adults in America alone – a developed nation – die of diseases that would never had affected them had they been vaccinated.
OR
2) There is not enough conversation between scientists and ordinary people about why things are necessary and what different studies mean (or the studies don’t get publicised enough) because doctors/scientists don’t communicate well enough with the wider public and the public can’t get access of easy to process information.
Likely, it’s a combination of both.
The question now becomes:
How do we fix it?
Well, to stop the anti-vac campaigns, we need to raise awareness. Make videos like this, blog posts like mine that expose these campaigns as the frauds they are go viral to the people who don’t know better and the people who question the necessity.
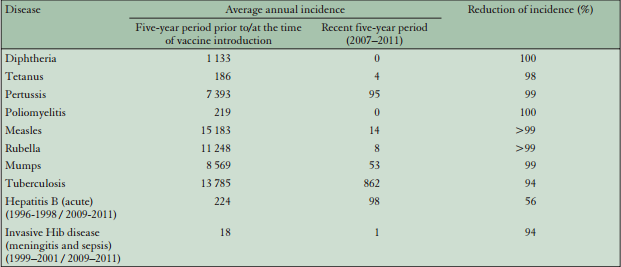
Vaccinations are why we, in the developed world, don’t have to worry about diseases like polio, smallpox and measles. 2 of those 3 still plague the developing world, by the way, and kill MILLIONS of people, a lot of them kids, every year. To make sure they’re effective, a certain percentage of the entire population needs to be vaccinated. This level, which we call “herd immunity” will ensure that the population can’t spread the disease that’s being vaccinated against easily. The number varies among different diseases depending on how easily it spreads and other factors, but for the flu vaccine in Australia this year, that number was 95%.
And if you’re skeptical about the effectiveness of these programs, a few of these stats should indicate how important they are.
Reduction in vaccine preventable diseases after 5 years of vaccination in Croatia:
Bernard Keich, “Impact of Vaccination on Vaccine Preventable Disease in Croatia”, Periodicum Biologorum Vol 114, No 2, 141 – 147
So they are necessary. And you can see from that video and my data above, they DON’T cause autism, like some groups would have you believe. They do have side effects in some patients (less than 1%), but most of them are minor, and they save more than they harm.
Without them, we’d still have millions of people, most of them KIDS dying every year.
Millions of kids die every year in the developing world from diseases that could have been vaccinated against.
We are privileged to not have our kids torn away from us.
But this may soon be changing… with incidences occuring more and more in developed countries due to the influences of the Anti-Vac movement.
You and I can stop this trend where it stands.
If We Vaccinate Our Kids.
You can do your part by sharing that video, or this blog post with those less aware than you so that you can save your kids’ lives, as well as THEIR KIDS’ LIVES.
My facebook page: https://www.facebook.com/musingsofamedstudentpatient An addition to the original post – A guide to educating those who think vaccinating isn’t safe:
One question to pose to all anti-vaccers next time you debate them – what’s the harm of vaccinating? The only evidence of it having some conceivable harm was the fraudulent Wakefield studies shown above. No heavy metals are added to vaccines any more by law, indeed, they never exceeded the amount you get in a serve of tuna. Risks of things like Gullian Baree Syndrome are 3/1,000,000. For the Flu vaccine, these rates are 1/1,000,000. The Flu itself has a 17/1,000,000 risk of causing GBS!. Risks of febrile seizure are present, at 30/100,000 children vaccinated, but they cause no long term harm. Indeed, reducing incidence of severe diseases like measels, or the flu, which cause febrile seizures at much higher rates than vaccines ever could, actually leads to LESS overall febrile seizures from occurring than vaccinating.
Common Arguments They Make. Why they’re wrong:
They often argue “It’s good to have some diseases early in life!” – well vaccines work on that same principle.
Except instead of giving you one that can leave you sterile, brain damaged or dead, it gives you a weaker/dead version of the disease so that your immune system is prepped for later encounters with disease. This video outlines the immune processes that occur in vaccination and the dangers of not vaccinating really effectively!
“They don’t work in all people! Why should I get mine?”
That’s true – they don’t always cause the intended effect, and vaccinated people can still get sick. However, if enough people in a population are vaccinated (and evenly so – as in, there aren’t pockets where people have very low vaccination rates where diseases can spread) the disease can’t spread in the first place, so everyone’s gotta do it for it to be effective. Many people (pregnant ladies and immunocompromised people for eg) can’t get them – so you’re protecting not only yourself and your kids, but also them. That’s the concept of herd immunity!
“But what about the toxins and insets on vaccinations which outline worst case scenarios and the vaccination court? Doesn’t that PROVE vaccines do cause harm?”
In preparing vaccinations to ensure they’re safe, some chemicals are added to some vaccines. The most common ones espoused by anti-vaxers are things like formaldehyde and mercury. However, you get 10-60x more formaldehyde when eating an apple as compared to the traces of formaldehyde left in vaccines after their preparation. Similarly, the use of thimerosal has also been criticized, but most modern vaccines no longer have ANY mercury or mercury derivatives (indeed, many of these mercury derivatives are passe through via stool as well) – and you get a higher dose of mercury in an 85g serve of tinned tuna than you do from any vaccine too.
“But can’t vaccination make me sick?”
Most vaccines out in the market are inactivated ones. The flu vaccine is the most famous, common example. Viruses are killed and there is literally no way that they can cause you to catch the disease. Live vaccines are out there too. But they utilise a severely weakened version of the pathogen they’re immunising for, or even, in some cases, use similar viruses or pathogens which are nowhere near as dangerous as the actual vaccine, but confer good rates of protection nontheless.
I understand. You’re concerned. But hopefully I shown you why vaccinating is so crucial. Do let me know if you are still concerned – you can reach me at info [a.t.] nikhilautar.com
Through my journey to recovery, I’ve said thanks countless times; to my doctors, my nurses, my parents and my bone marrow donors. But the other day, I realised that I must have had at least a hundred bags of blood pushed into my veins at some point in my treatment. That’s on top of the two very vital bone marrow transplants I had.
It’s staggering the lengths our health system will go to in order to save a life.
I guess only after getting sick and really needing those bags of blood did I understand the importance of blood donation. After volunteering at the blood bank, I realised how much goes into just maintaining proper stocks.
Most blood products have to be collected on a regular basis, as they can’t be frozen. In fact, all of them can’t, except for plasma. And, as you’ll learn by the end of this… some common treatments require literally THOUSANDS of plasma donations per patient.
I’d been brought up with the idea, the common misconception, that giving blood is a painful, time consuming process. But in truth – it was anything but.
I watched people walk in out within twenty minutes, smiling the whole time. Only 6 of which was actually spent giving blood. But despite all the great work that thousands of Australians, and those in other countries of course, do every day in donating blood – there is still a critical shortage. In fact Australia, as a country, still has to import blood to keep up with demand.
Only 1/30 people donate. These guys often donate regularly and are the reason we don’t have to import huge amounts of blood. People don’t give because they’re afraid of the procedure, because they don’t think it’s needed, or because they don’t care.
But what if it I told you that the only pain involved was the initial needle prick… pain no more than a blood test? That it only took 6 minutes. That there is indeed shortages in giving blood, and in the bone marrow donor registry, particularly in the minorities, and during winter when regular donors get sick. And what if I told you that there are pretty awesome benefits of giving blood too – you get paid, you reducing your risk of major diseases like cancer and heart attacks and you even lose quite a bit of weight losing weight. So you’re not only saving 3 lives every time you donate… you’re helping yourself too.
Well – all of these are true. And I hope these ideas will make you see that you can’t afford NOT to give blood.
1) It’s needed – and demand for it is always increasing.
2) It’s an easy, almost painless procedure.
3) It’s a free health check-up every 3 months and there are HUGE health benefits to boot!
4) There are financial benefits and free stuff that you could
be missing out on!
5) It’s a great way to lose weight and you get a guilt free meal each time you do it!
1) The necessity is
ever present and ever increasing.
Everyone’s heard this stat. 1/3 people will need blood in their lifetime. But only 1/30 donate regularly. As an Australian, as citizens of a developed country, we will never have a shortage of blood as we are rich enough to buy blood in times of shortages. Health systems suffer and people literally die when they don’t get access to the blood they need and to boot… that money doesn’t come from nowhere. We pay for it. Through our taxes.
Blood donations have to be constant. As I said before, you can’t freeze whole blood or platelets. And during cold and flu season in particular, regular donors are often sick and can’t donate – so it’s needed even more then!
So make sure you donate. The procedure takes, in most cases, 5-15 minutes. And almost all of the pain you feel comes in the first few seconds. They’re often less painful than even a blood test, because staff there do this every day, and because they have access to ultrasounds and other tech which makes the process less painful, and extremely accurate.
And the increase in the amount of bone marrow transplant procedures done, as doctors realise it is a viable method for treating a variety of autoimmune conditions, such as diabetes, scleroderma and even AIDS, as well as blood cancers like mine, means that demand for bone marrow donors is higher than ever before. But the registry, where your ’tissue type,’ (your immune profile – which has to match, or nearly match, a patients’ own profile to be able to do a stem cell transplant) still remains sparse. This means many people will not get a second chance at life like I had. In Australia, you need to donate blood to join the registry. And you need to actively ask them in the pre-donation interview to join it! So do that! In many countries, you only need a swab of the cheek!
But did you know, despite the scary name, over 95% of people who get called up to donate marrow (a 1/400 chance of that even happening) never actually have their marrow invaded at all? They need your STEM cells, which they can collect peripherally, from veins in your arms. I’ll explain how the stem cell donation process works more in the next section.
Sadly, some cultures in particular lag behind others when it comes to joining a stem cell donor registry, and giving blood. People of Indian, Asian, Black or Middle-Eastern descent in particular have much lower rates of participation on this front. This pie chart above, based on the American Bone Marrow Donor Registry, demonstrates this shortage for Asian and African-Americans in particular.
A lot of this is due to cultural beliefs that blood is related to male virility, but a much larger part of this is due to lack of awareness, or being afraid of the actual procedure. Well, hopefully, the next point will change your mind about that.
2) It’s easier than you think and involves little risk to the giver.
Many people relate the process of giving blood to intense pain and a lot of sacrifice on behalf of the donor. While it is a very noble thing to do, it’s not nearly as scary as it seems…
Did you know, whole blood donations are done in 6 – 10
minutes?
Did you know that the only pain involved is the initial jab
from the needle, not from the blood leaving the arm?
And did you know that a vast majority (over 95%!) have absolutely no side effects from giving blood?
I won’t kid you, the needle is larger than most. But the fact that you’re required to drink a litre of water before donating, and the fact that you’ve got the best phlebotomists (the fancy word for blood takers) working on you means your chances of having severe pain from a blood donation are very small. In fact, in his greater than 20 years experience in donating blood, my father has only had one “two-arm-specials,” where they had to jab him twice. IN OVER 200 DONATIONS! I’ve had a MUCH higher rate of blood takers missing veins in my 12-13 years of treatment, that’s for sure…
That alone is a true testament to the skill these guys have. As a doctor, I wish I had this kind of skill.
Here’s a picture to put it in perspective. The one they use in blood samples is the blue or purple one standing up. The one they use in taking blood donations is the light blue or black one lying down. Yeah, it’s a little bigger, but when you know that the pain only lasts an instant, not throughout the whole donation, it doesn’t make much of a difference.
Relaxing during a blood donation. Over 200 (300 now since I wrote this) done by this man – my father – alone.
Joining the bone marrow donor registry doesn’t involve extra
pain. In fact – they NEVER need a sample of your bone marrow to join!
To join the registry in Australia, historically, you’d have to donate blood and be under the age of 45, so that if a match is found, you don’t get the unfortunate situation of a person refusing to donate their stem cells due to fear of the procedure. Even then, joining the registry only involves the taking of an extra 20mL of blood, which they use to figure out your “tissue type,” which is used to match the recipient to a donor. You may as well, while you’re donating blood anyways, right?
When you consider you’re giving 475mL of blood at the time anyways, that isn’t too much. Make sure to ASK to join the blood donor registry, as they may not bring it up with you otherwise, and someone will hand you a form to do just that.
Once you’re on the list – you’re on there forever. And
there’s only a 1/400 chance of being a match for someone in your lifetime.
And the procedure of donating marrow is nowhere near as painful as it sounds! In 95% of cases, it’s actually STEM CELLS that you donate. The process takes 3 hours and basically involves taking blood from one arm, siphoning off the stem cells they need, and pumping it back into your other arm. They may give you medications a few days to weeks before to ensure your stem cells exit your marrow, and circulate in your blood.
But even if they need to take it from your marrow, you’re under general anaesthetic, so it’s nowhere near as painful as it sounds. In fact, that 5% of people who do give via that means, often do so because they’d prefer to not feel anything and take a while to recover than choosing the other option.
For more info on how to join the registry, click here:
3) It’s healthy for you! You get a free health check-up. And it may reduce your risk of heart disease, cancer and diabetes too!
Every time you give blood, they need to assess whether your blood is healthy. So giving blood every 3 months is essentially a free, quick health check-up, at least for your blood counts (though I wouldn’t recommend not getting physicals/check-ups done just because you’ve given blood). It’s a great way to catch diseases early.
Indeed, in my case, I would’ve known I had myelodysplasia syndrome (MDS) a long time before it developed into its deadly form, acute myeloid leukemia (AML). And MDS is much easier to treat than AML, which I found out the hard way.
I’m not saying that you’re at risk of getting such diseases if you don’t give blood, but you will definitely pick up on any abnormalities you may have earlier, making any conditions you may develop much more easily treatable if you do.
4) You’re missing out on a lot of benefits – including time off, and money.
While talking to a few donators at the marrow centre, I realised that a lot of them were there not only to give others a second chance at life, but also to help themselves fiscally.
A lot of the donors were actually school kids. I wondered why. Apparently, they came as often as they could over the year in order to miss a few periods of class.
But it’s not just school kids who benefit. A good chunk of people donating were actually being paid to do so, or given a half day, or day off by their employers. There are many schemes and benefits out there where you can donate blood and actually be paid for the time it’s taken out of your day by your employer. And I’m sure sitting in a chair for 10 minutes is much more preferable to slugging it out at work! Depending on where you live, there may be tax benefits eligible for donating.
Indeed, in some countries, including the US, they even pay you for donating blood!
Here’s a link to a video of how you can do this in America:
The ethics and implications of a system which compensates everyone for donating is interesting. But if you can cash in AND save lives, there’s nothing wrong with doing both!
Feel a split second of pain in your arm and sit on a chair for under 10 minutes or run 4-5 miles? You decide.
I know which one I’d choose…
Not only that – but after giving blood, you’re given a chance to go crazy over a veritable buffet. At the centre where I volunteer (Liverpool) there are sausage rolls, pies, soups, milkshakes, coffees, toast and more – and it’s served by chirpy, good looking volunteers (well, at least when I’m on duty).
When I’m feeling too lazy to cook one day, or needed a break while stressing over exams, this would be where I’d be going to get a free meal. Indeed, the fact that you know your body will have to work to make up for what you’ve lost will mean you can have a guilt free meal. Be warned though – too much donating can result in a figure like this:
Dad going to TOWN on some freebies. Remember – this is only the COLD food they provide. Add to this sausage rolls, pies and milkshakes, and that’s what’s on offer every time you donate! Some centers have other meals on offer too, including lasagna, pies, and even give out additional meal vouchers for restaurants.
So – now that you’re convinced that you’ve got to go out and give blood – remember these things:
Before giving blood, make sure you have a meal and drink a litre of water within 3 hours of donating. It’s a requirement and you don’t wanna be turned back on the day! Try and include high iron foods and things like orange juice (which increases iron absorption) to ensure your iron and haemoglobin levels are sufficient. A tip from the nurses there – spinach and orange juice in the meal before you donate increases iron levels into the healthy range for those who find themselves turned back for being too low. My mum had low haemoglobin levels, and was turned back many times when trying to donate. But after eating that spinach with orange juice (she’s a vegetarian, so red meat wasn’t an option) religiously for a few weeks, she managed to donate blood for the first time during COVID-19 lockdowns – when it was needed most!
Make sure you haven’t travelled to areas with infectious diseases in the past 3 months and make sure that you can prove any recent tattoos you’ve had were done in sterile situations.
After you’re done giving blood – make sure you drink a glass of water before eating or drinking anything hot, just in case, as it reduces the already small chance of vaso-vagal syncope.
To find and make an appointment to give blood at your local blood donation centre, click here:
Unfortunately, a small chunk of women, and some men, can’t donate blood as their iron levels are not high enough. And there are other reasons why people can’t donate too.
But if you can’t give blood and join the bone marrow donor registry, you can still spread the word and encourage others to do so! Whether you mention it next time you catch up with friends or just post it on your Facebook wall – these things all count and if it helps 1 extra person get into donating blood, well, you’ve already saved 3 lives!
If you are donating – make sure you “check in” on social media each time you give blood. Letting people know what you’re doing is not boasting (even though it’s definitely something you should be proud of) when it gets others to donate too!
You can also volunteer at the Red Cross like I do, either by helping out and giving snacks to the donors, or by driving a car or van that picks up donors. It looks great on your CV and you’re just as vital a cog in the great machine as the donors themselves. Click here for more info.
Participating or donating to people in the World’s Greatest Shave or events like the Leukaemia Foundation’s “Light the Night Walks” also helps in a similar way.
Here’s a speech I gave at the most recent Light the Night event about how I stayed happy during my treatment, and how the Foundation helped me during my treatment:
Other things you can do include donating to the Red Cross or
to the Leukemia Foundation, which can be done through the links below. These organisations are trying to find a cure and save people from having to go through this pain in the
first place!
And make sure you share this with others and on your Facebook Walls so as many people as possible join up and so more lives can be saved.
Another way you can donate – PLASMA! And why it’s so necessary!
The name of a treatment I used to get – Intragam. Not Instagram. #INTRAGAM.
This was a blood product I used to get once a month to help with the chronic inflammatory disease process and nerve damage my#bonemarrowtransplant gave me. Though it wasn’t fun, coming in every month to be plugged into an IV pump for over 2 years, it likely did delay further damage and was one of many blood products which have kept me here.Every 200mL bottle takes 7.5 ENTIRE Plasma donations to create, if we’re strictly speaking numbers of immunoglobulins, aka antibodies, specifically IgGs (antibodies essentially confer immunity to people who can’t produce antibodies on their own, and mitigate some autoimmune disease processes by triggering suppressive pathways of your immune system) per mL, dosage wise. I used to get around 750mL of this stuff. Every month.But each of these bottles contains a mix of 1000 individuals’ IgGs. It took a literal village to keep me going for a time there! And plasma, like blood, is not only easy to donate – it can be done every 2 weeks, and, as you can clearly see, is really needed.More info on that process, on how easy it is to donate blood, how it actually is healthy to do so (each plasma donation burns 450 calories – whole blood, 600!), and how joining the list to donate bone marrow (and even donating bone marrow itself) doesn’t require, at any point, a needle in your bones at nikhilautar.com/donateblood #redcross#vampirecup#blooddonation #intragam#notinstagram#everydonationcounts#doit!#spoonies#spoonie#chronicillness#chronicpain#nervedamage#peripheralneuropathy
2 years ago, to this day, I received a bone marrow transplant.
It was the hardest thing I’ve gone through, as a cancer patient.
I spent weeks stuck in a bed, subsisting on unsolid food, barely drinking and in intense pain – even with morphine!
And for months after it, I was fed into a spin-cycle of maladies, starting with my skin feeling like it was burning for days on end without relief, followed by months of sickness and huge shifts in weight and ending with the a relapse and the knowledge that I’d have to go through it all again in my second transplant.
But it saved my life.
And I’m eternally grateful for it and for my donor.
One thing that may astound you is the fact that the transplant took only thirty minutes, didn’t involve any pain – it was just a minor, drip-like infusion!
Even DONATING bone marrow doesn’t mean having a needle put into your bones these days – at any point!
Bone marrow transplants are the cure to variety of illnesses – not just blood cancers/disorders which I speak about mainly on this post.
It has cured AIDs, which has only happened twice, EVER.
And it’s the only way possible for a mammal to change blood types.
Personally, I’ve had 3.
Click here to skip to a particular section of this post:
How it works
Finding a Match
How YOU can become a donor
What happens to the donor
What happens to the patient
How It Works:
So how does it work?
Basically, a bone marrow transplant, also known as a haematopoietic stem cell transplant, replaces your old bone marrow with someone else’s. You can also use your own cells for this, but for this post, I’ll only talk about allogeneic transplants, ones you get from other people, rather than autologous ones which you get from yourself.
Bone marrow is the soft, spongy tissue inside your bones which make your blood. It’s usually filled with haematopoietic stem cells – cells which rapidly divide over and over again and transform with the aid of certain hormones and chemical messengers produced by your body to eventually become your blood cells.
When a disease process affects these stem cells, they cause a malfunction in your blood cells which has a wide range of complications as your blood is responsible for delivering oxygen and nutrients to your body, and also your immunity, amongst other functions. If that disease involves a change in the actual DNA sequence of the stem cells and divide so it begins to take over the normal stem cells (in other words, if the disease is a cancer) and chemotherapy is not an effective cure for it, then a stem cell transplant can become the best curative option.
Now here, I wanna make it clear what I mean by “Bone marrow transplant” in this post. I’m referring specifically to Allogeneic bone marrow transplants – one received from SOMEONE ELSE. It’s possible to have an Autologous BMT too – in a procedure where your own blood stem cells are collected, so that they may be injected back into you after treatment. This is usually done to get very high doses, or treatments that would otherwise have killed off your vital bone marrow for good, into a patient, without killing them. The collected cells are stored and injected back into the patient after treatment has taken effect and remnants of the drugs have left the body.
What an allogeneic stem cell transplant does is get someone else’s bone marrow, blood producing cells into you. Not only does that allow for, if required, the same high doses of chemotherapy and other treatments to be given, it also gets someone else’s white cells (white cells are blood cells, made in the bone marrow) into you – their immune system. And this had the added effect of them attacking your cancer cells, where your old immune system couldn’t (often, cancers have special mechanisms by which they can evade your immune system), or of getting a new immune system in there to replace the old one.
The Procedure:
An allogeneic transplant involves, on the patient end, first, some chemotherapy and radiation to the entire body (blood production, though often limited to bigger bones like your sternum or hip bone in adults, can occur in any bone in the body) to ablate, or kill off, your old, diseased stem cells. Less intense chemotherapy regimes can also be given, in diseases with lower agressiveness or in patients who can’t take as much of a battering (my second transplant, due to all the drugs and radiation I’d had previously, was done using a “reduced intensity chemotherapy” regime. Many older patients are now able to get bone marrow transplants where they weren’t before due to these regimes).
The major side effect of this step is that your blood production halts, or stops outright, meaning you will be much more likely to bleed and bruise in that period and be very susceptible to infections – which are even more life threatening as you don’t have white cells to kill them off. Many of the drugs also have side effects of chemos (they often are chemos), and the radiation itself can cause severe mouth ulcers in some. This in itself makes the procedure very risky.
After this is accomplished, you inject your donor’s stem cells into your body in order to replace it. The donor’s stem cells take around 3 weeks to engraft, or take residence and begin working, in your bone marrow and from then on your donor’s stem cells become your own. Which means that from now on, you’re producing YOUR DONOR’S blood cells instead of your own.
The intent is not only for his (or your donor’s) cells to take over and start making proper blood cells again, but also to stop your old stem cells from coming back. You see, when his cells take over, his immune system does too. This is what is trying to be achieved in the whole procedure actually, a change in the immune system – as his immune system, being different to yours, will, hopefully, kill off any old stem cells of yours (including your cancerous ones) that remain. This is called the Graft Versus Disease effect (GVD).
The problem is, there is also a good chance that his immune system will also find your body’s other organs to be foreign to it and it will attack them too. This is called Graft Versus Host Disease (GVHD). And it is a big reason why it’s seen as even riskier than even chemotherapy and radiation.
In order to reduce the impacts of GVHD you are given some immunosuppresive drugs, which, as the name suggests, suppresses the immune system. When given early, it also prevents your old cells from coming back from the radiation and chemotherapy to cause rejection.
Examples of these are methotrexate, and cyclophosphamide, given before transplants to reduce both the risk of acute GVHD and the chances of your immune system from rejecting the donor’s stem cells, cyclosporine in the long term to manage chronic GVHD (GVHD that presents 6 months to years after a transplant) and prednisone, a corticosteroid, to manage acute GVHD (GVHD that presents after engraftment. Prednisone can also be given long term to manage cGVHD, and many of these drugs are used at different points).
GVHD can be life threatening, if not managed well. GVHD is a big reason why a transplant is seen as a very risky procedure. And though acute GVHD is more dangerous, chronic GVHD can have long impacts into the future.
But it’s not all bad news. Actually, the presence of GVHD and having a more severe version of it is correlated to a higher cure rate because the GVD will also be stronger. It’s a balancing act. You don’t want too much severe GVHD but a little bit is good as it indicates a good level of GVD (graft versus disease) as well.
And if you catch GVHD fast, and do as recommended by transplant hospitals, and rush to emergency, or call up your doctor immediately to initiate treatment in the critical periods (up to 3 months after a transplant, or when you feel classic symptoms of GVHD like fevers, gut pain/diarrhoea, skin prickling/redness/rashes or eye dryness. It can affect many other organs in different ways too) – it is often gotten on top of!
Finding a match:
When you’re being matched to your donor, it’s very preferable to have a complete HLA match. Basically your HLA is how your body recognises and differentiates your own cells from that of other foreign cells. You inherit your own ‘HLA settings’ from your parents, half from your mum and half from your dad and there are many HLA subtypes people can have, making it very unlikely for two random people to be matched to each-other.
Usually there are 6 main subtypes they look at when they’re trying to find a donor to match for you (they can go to 8 or 10 or more as well – I was a perfect 10/10 match for HLA with my donor). You have a 1/4 chance of any sibling being a match for you. In fact, transplants from siblings get lower amounts of GVHD, so they’re seen as less risky (by the way – even being a 10/10 will result in GVD and GVHD occuring, as there will always be little differences between your donor’s immune system and your own). But outside of your immediate siblings, the chances are very low due to the sheer number of possible HLA subtypes combinations that there are. But they do happen.
That’s where the bone marrow donor registries come in.
How you can become a bone marrow donor:
Bone marrow donor registries are usually done by country. It’s basically a huge database of people’s HLA combinations.
The process of actually joining the registry varies from country to country but NOT ONE involves too much pain! NOT ONCE will you have to get a sample taken from your bone marrow! What they need is a tissue typing test – a test which checks which HLA subtypes you happen to have.
In the United States, this involves simply buying a $5 test simply taking a swab of the inside of the your mouth and sending it away. In Australia, it involves a 20mL sample of blood, and has to be done while giving a blood donation (which takes less than 10 minutes and is no more painful than a blood test by the way) – and you have to ask and fill out a form in order to do it. This is done to ensure that everyone on the registry will be willing to actually give the donation. In the US a lot of people opt out of actually becoming a bone marrow donor in fear of the procedure, so finding a match doesn’t equate to finding a donor, which it usually does in countries using Australia’s approach.
With the help of my doctors, I was extremely lucky to find 5 matches, from around the world, and have had 2 bone marrow transplant from them.
Only 60% of people can find one.
So we need you to join up on the registry. Especially if you’re from an Asian or Indian or Middle Eastern background. It is more preferable to find someone who’s similar to you – whether it be by race, gender or age, and these races in particular have critically lower rates of people joining the registry.
Find out how, if you live in Australia, by clicking the link below:
The actual procedure rarely ever actually requires harvesting of actual bone marrow either (95% of the time it doesn’t and a good portion of the other 5% choose to go through the surgery process because they have access to general anesthetic through that pathway). The donor has to go through a series of subcutaneous injections, small injections under the skin – usually into the belly or arm, of a hormone which increases the activity of stem cells and causes them to enter the blood more. From there, blood is collected from the donor from one arm, siphoned through a machine which separates the stem cells from the regular blood, and the regular blood is injected back into the patient’s other arm.
There is a chance that you’ll need to have surgery to remove actual bone marrow from your bones as well. Though it is unlikely nowadays, the procedure is done under general anesthetic meaning you won’t feel pain from the operation, and is very safe too.
The procedure for the patient:
The actual transplant is a bit of an anticlimax. The stem cells, collected in a bag, are infused into you, just like a saline drip, except with blood. In some cases, or in cases where a complete match wasn’t found, you can get a reaction to the actual cells.
What is dangerous during the procedure is the chemotherapy and radiation which kills off your original stem cells.
As with any systemic chemotherapy, your fast-growing cells are killed off. This includes not only your bone marrow, but also things like your hair and the lining of your gastro-intestinal tract. This leads to very low blood counts and hence tiredness, very low immunity and higher chances of bleeding, as well as abdominal pain and diarrhoea or constipation. There are a range of other side effects too such as nausea and taste changes which aren’t pleasant to say the least – but all of these can usually be controlled with medications.
The low immunity in particular is of huge concern. Your neutrophils, the white blood cells at the front-line when fighting infections, plummet to 0 and not only do you become more susceptible to infections, you also become very weak at fighting them. In fact, it’s the leading cause of death in not only bone marrow transplants, but also in chemotherapies and even in hospitals. Hence it is important to stay away from other people who may have infections during a transplant, and also important for appropriate hygiene measures to be taken, such as always sanitising your hands before allowing others (including doctors and nurses) to touch you and being placed in a room where the air is always being filtered.
Often, despite these measures, you can still get infections from your own body – it’s something you can’t help. These usually manifest as fevers or shakes or coughs and the like and are treated very aggressively, as your body has little to no capability of fighting them. Don’t worry though – medications can take the place of your immune system while it’s weakened – so infections are mostly controlled if caught early.
The total body irradiation is another factor which comes with a range of side effects. The procedure itself is a little daunting at first, involving being beamed with radiation for 20 minutes whilst being placed in a box and held still by rice bags, but after a few times (it’s done once a day on a 5-7 day cycle), you get used to it.
Again, it will cause your blood counts to drop and subsequently cause the cascade of side effects that come from that but it also causes skin irritation and in particular, mucusitis – or pain in your mouth and throat which, in my transplant, was the worse symptom. I found intense pain on swallowing – even if it was water or my own saliva and hence spent almost 3 weeks eating little more than less than a tub of gravy or custard and little sips of water. A morphine pump wouldn’t even help with the pain, and the sad thing is, 85% of patients who go through total body irradiation get this. But there’s a way around this too – a nasogastric tube which allows for food and water to be pumped into your body rather than forcing you to swallow it through a very sore throat.
There are also other ways of doing transplants which don’t involve the radiation aspect of it – and my second transplant is an example of it. It was a transplant whose pre-conditioning only involved chemotherapy(and that too a less intense variety of it) protocol known as RIC (Reduced Intensity Chemotherapy).
Bone marrow transplants are complicated, often risky procedures. They’re hard and often scary, and unfortunately necessary for some. But they give a second chance for people facing cancers, and other blood related or autoimmune diseases, at life.
I can never be thankful enough to my 2 donors for what they’ve given me – a total stranger – to them. And they haven’t asked for anything back from me.
They’re angels.
I hope for a day where no-one has to go through the things I went through during my bone marrow transplant. ‘Til that day comes though, be sure to join your country’s bone marrow registry and become an angel yourself.
Those from other nations (though this is aimed at professionals, you can search for your nation, and find organisations that have and contribute to registries there):
You see it all the time on those medical shows on TV.
You see a doctor, who could probably earn millions modelling
on the side, running through hallways and corridors, hanging IV drips, getting patients
food, finding time to sit down and talk patients through all their fears and
concerns – basically doing anything and everything to help the patients through
all of their troubles.
I guess that’s what I’d expected would happen when I was told I had cancer.
My first week in hospital, however, would turn out to be a shock to my system. Even on the
day I was diagnosed, I saw my doctors for no more than thirty minutes. 30
minutes! And that would turn out to be the longest single session I’d see a doctor in
a day, outside of emergencies… well… ever.
In the end, it was the nurses who did the REAL work.
I’d been brought up, maybe through the media, maybe through cultural
perceptions – probably through ignorance – thinking that a nurse was just an
over-hyped house-maid.
As it turned out, it was a nurse who placed my first canula
in emergency. A nurse who took my bloods every morning. A nurse who’d be in
charge of injecting chemotherapy through my central line – a long plastic tube
that pumps medicines from the veins in your neck to your heart. Hell, it was a nurse who
put that in too!
If it wasn’t for their badges and uniforms, I wouldn’t have known the difference between them and the doctors.
In fact, I would’ve thought that they werethe doctors.
Because the thing I found most astounding was that despite all their work on top of these vital responsibilites, despite taking care of, at times, half a ward-full of critical patients… despite their unreasonable shifts and rosters, they still managed to find the time to do all those I thought doctors would be doing.
Yeah, it was a doctor first gave me the bad news. Yeah, he was the one who prescribed all my medications. Yeah, he was the one whose knowledge and experience I could trust.
But it was a nurse who sat down and hugged me with my parents that day after I’d been told I had leukemia. A nurse who told me that my journey would be hard, but reminded me that I could survive nonetheless. A nurse who would sit down and just chat when I just couldn’t find it in me to sleep for the pain and worry.
And no matter how many cards we gave them in thanks, no matter how many chocolates or donuts we brought in – the true testament to their generous, giving souls, was the fact that they ALWAYS shared them with all the staff on duty.
Personally, for me, they’ve always been the balm that eased the sore of treatment. The girls and guys who’d go beyond their strict professional duty and hold my hand in emergencies, keep me calm during procedures and just keep me cheerful through their words and their, at times, crazy antics.
And if it wasn’t for them, I wouldn’t be the man I am today.
I remember the day I came back in for my second round of chemotherapy. My heart was racing, pulse rising from my usual 60 beats per minute to well over double that, and it stayed that way for most of the day.
I was back in that damn place, stuck in the tiny confines of that room for what would end up being fifty-six consecutive, bed-ridden days. And the crazy thing was, I didn’t even realise I was in trouble. I hadn’t felt apprehensive or anxious about all this… I’d unconsciously bottled it all up.
But then, as I walked around the corridors and glimpsed the door of my last room, I saw this.
They’d known that I was a fishing tragic and that that was exactly what I’d be doing in my 2 week break. No matter how tiring, risky and stupid.
And, just realising that the next few weeks of pain and torture would be eased by these people, these amazing souls who made their job a profession dropped my heart rate back down to normal.
They’re angels, all of them. The humblest, most devoted, most under-appreciated, yet most vital aspect of hospital life. And in my eyes, they’re the lynchpin of our medical system.
So I hope after reading this, that next time a nurse tells you that you’ll have to wait another half-hour in emergency, you’ll understand it’s probably because there’s somebody who’s going through haemolytic shock due to
blood loss just behind that ED door. Next time a nurse insists that you leave a friend or family members bedside, after initially getting upset, you’ll see that it’s because if they didn’t, other patients’ rest may be in jeopardy. Next
time you’re about to berate a nurse for getting the bloods done a little late that morning, it’s probably because they had six other patients to medicate before they’d even gotten the chance to pull bloods out of a line.
And I hope that you’ll forgive them. If not for their compassion, dedication or graciousness, for the fact that you’d expect the same of them if you were the one on that bed.
Don’t worry – I know there are many roles in healthcare that
do just as amazing work – social workers, dieticians and the hospitality to give a few examples. I’ll be doing them justice in later posts, don’t worry about that.
As for doctors, I do believe they have to up their game in helping the people they care for beyond just their physical condition. Read more about that here https://www.facebook.com/musingsofamedstudentpatient <– If you or a loved one needs help or if you enjoy my blogs or if you’re interested in medicine, like this page on facebook =]