So I’ve been getting a LOT of questions about COVID-19, the name formally given to the strain of coronavirus that’s on the verge of becoming a global pandemic. I’m particularly concerned that there’s a LOT of horrible horrible misinformation being spread, and many trying to profit off of this right now – including, but not limited to – pastors trying to convince people to drink bleach to cure non-confirmed cases of the virus. But it can be really hard to get proper information on this virus and how to prevent infection and spread. Hence, I’ve put together this blog post which I’ll update weekly every Saturday for the next few weeks (less and less frequently over time as or if the burden of disease diminishes).

Pictured here, your average Karen, freaked out by the Corona-virus. Should she, though?
How Lethal Is It? – More lethal than the flu, but numbers will likely change over time.
The latest information we’ve gotten directly from, largely, the Wuhan Epicentre (the numbers come from the Chinese Centre of Disease Control and Prevention) of disease shows that out of 72314 cases studied, there was an overall mortality rate of 2.3%. No deaths have been recorded in those aged 0-9, but deaths do increase exponentially with age, which is to be expected with many viruses of this type (peaking at a 14.8% mortality rate in those over 80). It’s important to note that an association with healthcare burden and death has been demonstrated in this virus, with the epicentre and neighbouring towns in the area seeing much higher mortality rates, which basically means, mortality rates could be inflated, as Wuhan exposures did dominate in terms of cases examined here. Poverty as well could skew mortality rates further as well, as is the case with many diseases such as measles. But figures may be downplayed as most cases of disease are mild, and the fact that China’s numbers and reporting of this has been questioned by many.
Though sample sizes are low, as we approach a few thousand people surveyed, it’s likely that overall mortality rates are lower than what’s been seen in Wuhan and Hubei (the province which Wuhan is capital of). The most accurate coronavirus figures are updated regularly and most accurately by John Hopkin’s University.
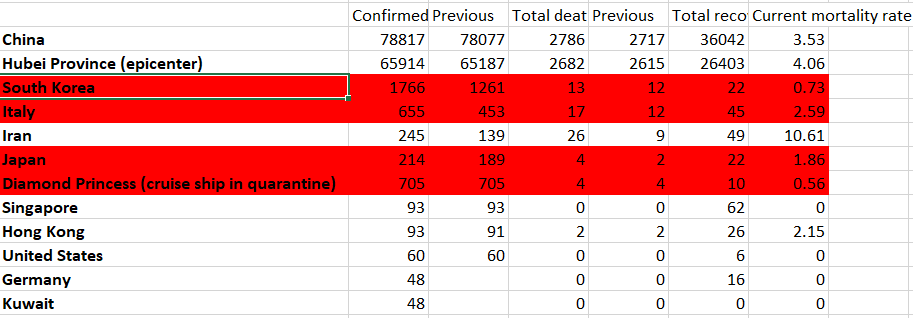
Important to note – Italy and Japan have both been ‘shocked’ by this outbreak and are now responding with vast restrictions, which should reduce incidence and cases. Iran, as you’ll see below, has not been following that example and has a notoriously bad health system to begin with, with some of the lowest number of hospital beds per capita in the world – fitting it directly under the low healthcare resources category described above.
What does Flattening the Curve Mean, and why do we need to control disease early?
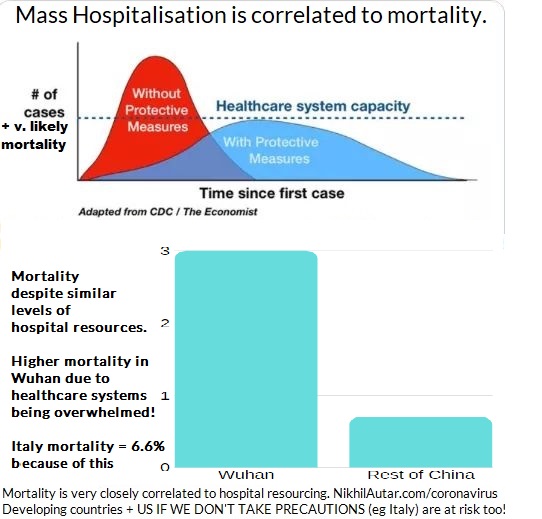
This summarises this best. But basically, the idea of making sure that both cases, and hence mortality, doesn’t exceed hospital system capacity is very important. As demonstrated above, there is a correlation between higher mortality rates and overburdened hospitals. Cases in Italy have been severe, to the point where doctors are being forced to make terribly hard decisions. If we stop the spread, however, we have the chance of not overwhelming hospitals and ICU beds and respirators, which are currently out of stock, and minimizing death.
I heard that China stopped the Spread. Can we do that too?
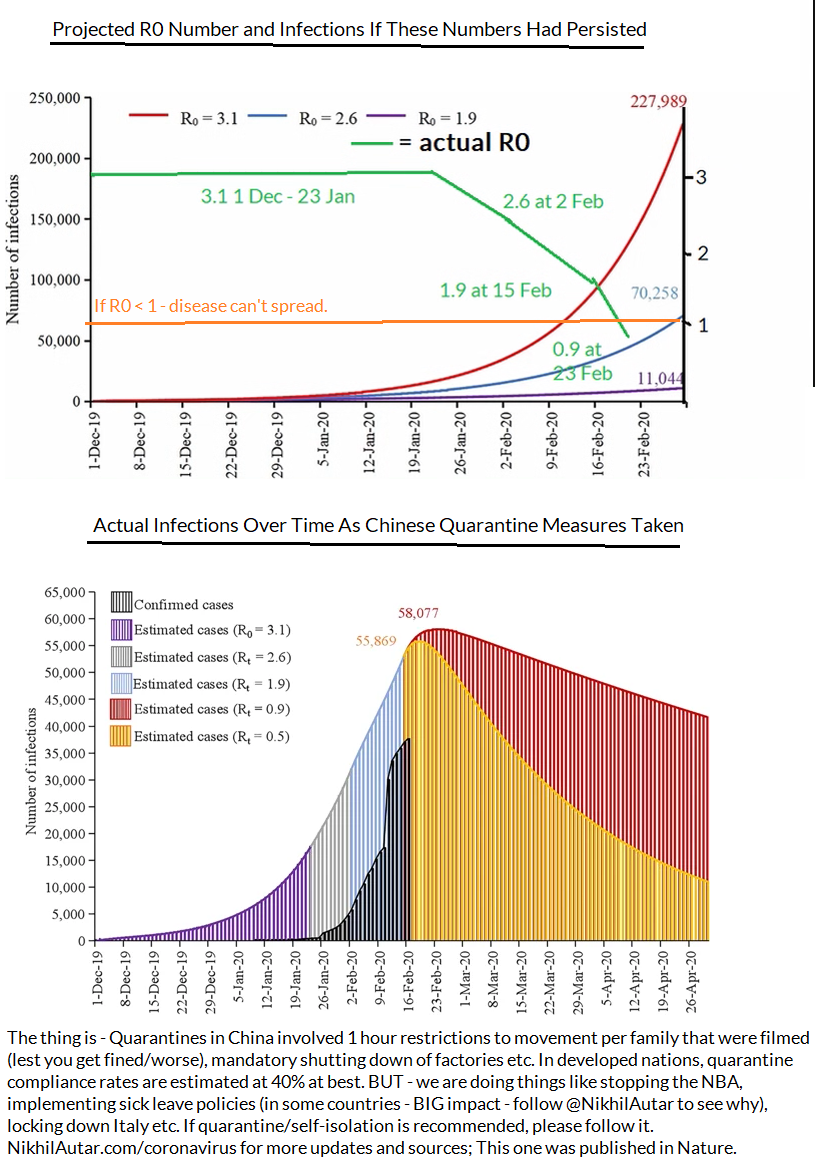
When the R Number reaches below 1 – disease can no longer spread. China has reached that point – but what remains to be seen if measures that Italy and other nations have taken can stop it in lieu of a vaccine which can help diminish spread or stop it altogether.
Outside of Age, are there any other risk factors? – Yes.
If you have preexisting conditions – the coronavirus could be especially dangerous for you, with mortality rates of 10.5% for cardiovascular disease, 7.3% for diabetes, 6.3% for chronic respiratory disease, 6.0% for hypertension, and 5.6% for cancer. It’s important to note that these diseases are often faced by older people and that these numbers weren’t adjusted for age in the study, but viruses do typically affect the already ill worse, so it’s very reasonable to assume there is a higher risk if you happen to fall under one of these categories.
How fast and far will it spread?
The “R Number” – R0 (the number of people you’ll infect, on average, if you get the disease) has been confirmed to be around 2.3, through a convenient study where 355 verifiably infected people managed to be in a confined space for a few weeks in a row – ideal scenarios for calculating this (which may, if anything, given it was done on members of a cruise ship which is REALLY confined) inflate numbers slightly. which makes it more infectious than the common seasonal flu, and even previous flu pandemics. It’s important to note though that these previous pandemics were in times when diagnoses weren’t high, and that other disease specific factors play into the spread, but though it doesn’t look high compared to other highly infectious diseases presented below – given disease characteristics and the lack of a vaccine, it’s definitely got pandemic potential.
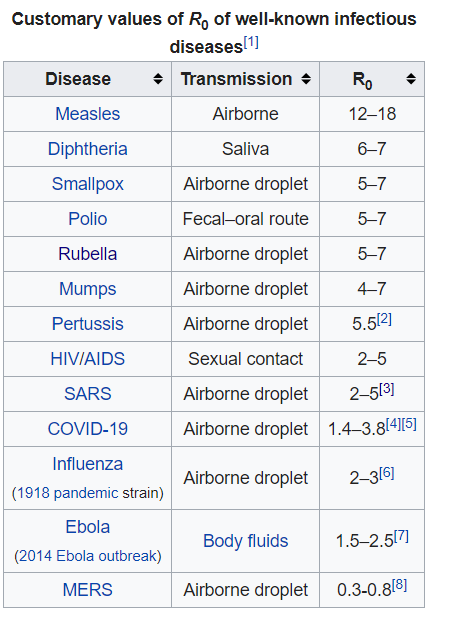
Unlike the diseases ranked higher than COVID-19, COVID-19 does not have a vaccine developed for it yet.
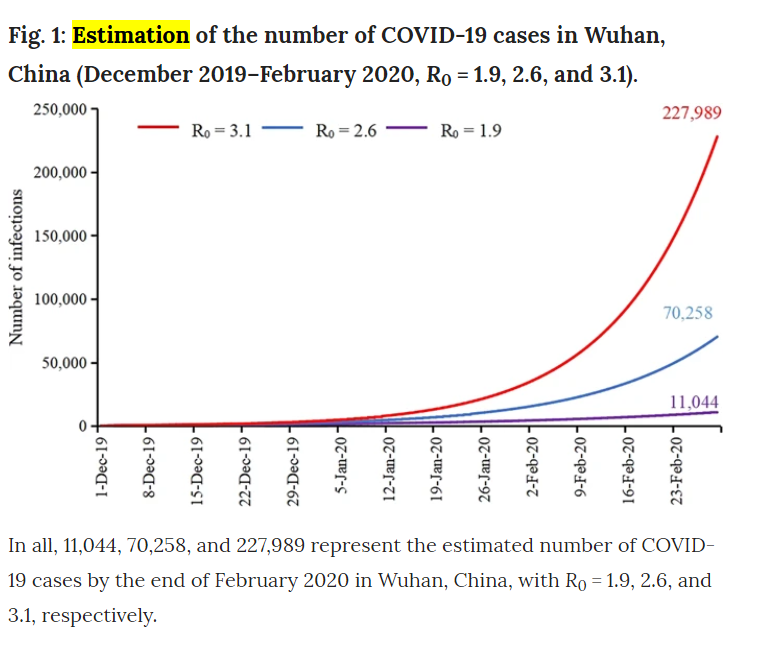
According to estimations made a few weeks ago (between January and Feb 15) on in the course of disease, there should have been less infections as there are now by the middling series of Rt estimates (in this study, they modeled data from January under projected number of cases and estimated that with a R number of 2.6, there should be around 70,000 by Feb 29. As of March 3, there are 80,000 cases in all of China. But with the interventions the Chinese government took, shutting down factories and effectively quarantining a nation, assuming a reduction in R0 as time goes on (which was observed by researchers), we should have peaked by now in terms of novel cases in this district.
Does that mean the spread is stopped? No – there were extreme measures taken in China and Wuhan in particular. But it could mean that R0 has been overblown thus far, likely due to endemic factors such as overburdening of healthcare resources, or poverty. We can’t know for sure right now – in any case, given its propensity to be more lethal
So what do researchers think is going to happen? Well, it’s hard to predict. But given that SARS and MERS, the 2 most recent coronavirus related pandemics we’ve faced, have been less community-spread than this strain of the coronavirus, and that there are numerous cases in the US popping up now where there’s been no contact between the patient and someone around them, there’s a higher chance of this spreading further than those other 2 did, but with lower mortality rates, it could be the case that this won’t be as serious. It’s great to see a coordinated global response behind this. But there are many instances of misinformation going around which is concerning to say the least. For example… it doesn’t help when thousands of pilgrims go around licking statues in Iran, the nation with the second worst outbreak of COVID-19, nor is it safe to go around, kissing people and making contact with random strangers in public, something the Pope insisted on doing despite Italy having the worst outbreak of COVID-19 (at the time of writing this) in the developed world.
Why? Surely Allah has better ways to test faith than challenging you to thumb your nose at what could be a global pandemic… As a nation which sees tens of thousands of pilgrims a day, and one already struggling to cope with the virus (indeed, it hasn’t got amazing healthcare, which, as we demonstrated above, is correlated to worse outcomes), it’s imperative we don’t do stuff like this.
Stopping Transmission And Reducing Your Risks
This is by far the biggest question I’ve gotten so far. Though some bodies are urging people to not buy masks and other personal protective equipment for the flu, mainly for supply chain reasons (practices in Australia are running low on supplies right now!), the evidence on whether or not coronavirus (or any virus for that matter), can be reduced in its transmission by things like masks or hand hygiene isn’t clear. There are several studies showing that transmission does go down with use of a more robust n-95 masks in healthcare workers who see this disease everyday. Medical masks aren’t shown to significantly improve rates of infection, but both treatment groups (those instructed to use hang hygiene, and those instructed to use hand hygiene and a mask) did see a reduction in rates of influenza compared to controls (yes, this was a highly reliable RCT, the only one I could find on this topic online). The facemask + hand hygiene group saw a 43% reduction vs 8% compared to controls with face masks alone, and none of the results were significant. But despite not reaching such large number, that same study ultimately concluded that these measures may help reduce rates of transmission, and that it should be recommended in crowded places during flu seasons.
Another study showed that in household studies, donning a mask, while also educating participants on the importance of handwashing, did reduce rates of catching illness by 67%. Most studies have shown limited benefits in either methods, but most studied also involved using various kinds of masks or hand hygiene after someone else developed symptoms, which may not be viable in diseases with longer incubation periods, which COVID-19 is looking like it will be (mean incubation period is 6.4 days from Wuhan epicentre case study analysis vs 2 days for most influenza strains).
Does that mean you need one if there’s no evidence of a major pandemic in your area? No. As there seems to be a global shortage – let those who need it most – healthcare workers who may be screening for this now – get their supply first if you’re well. But if you are a cancer patient, someone who’s got those comorbidities listed above (cardiovascular disease, chronic lung disease, diabetes or hypertension), I wouldn’t blame you for being cautious – especially if you’re going to hospital!
Finding a Cure
Another concern is media misinformation, and misinformation being spread by people on Facebook trying to make a quick buck off this epidemic. From that example of someone trying to sell bleach, to things you’ll see often in Twitter, or Facebook Groups everywhere, no – there is no verifiable cure for coronavirus yet. Research hasn’t demonstrated the virus is liekly to be susceptible to Tamiflu yet, but if you’re getting symptoms, and your doctor recommends it – take it. Though it may not be the easiest pill to swallow, it’s most effective taken soon after infection, and you could well have the flu which can be mitigated in its severity with Tamiflu!
Several homeopathic remedies have been suggested and are being sold to people on Twitter and in Facebook groups – don’t be fooled by the name. If it’s not being prescribed by a doctor, it likely won’t work, and you spreading that it could, could lead to people not getting seen by doctors, being diagnosed and properly quarantining themselves for one. Be very careful with what you say online!
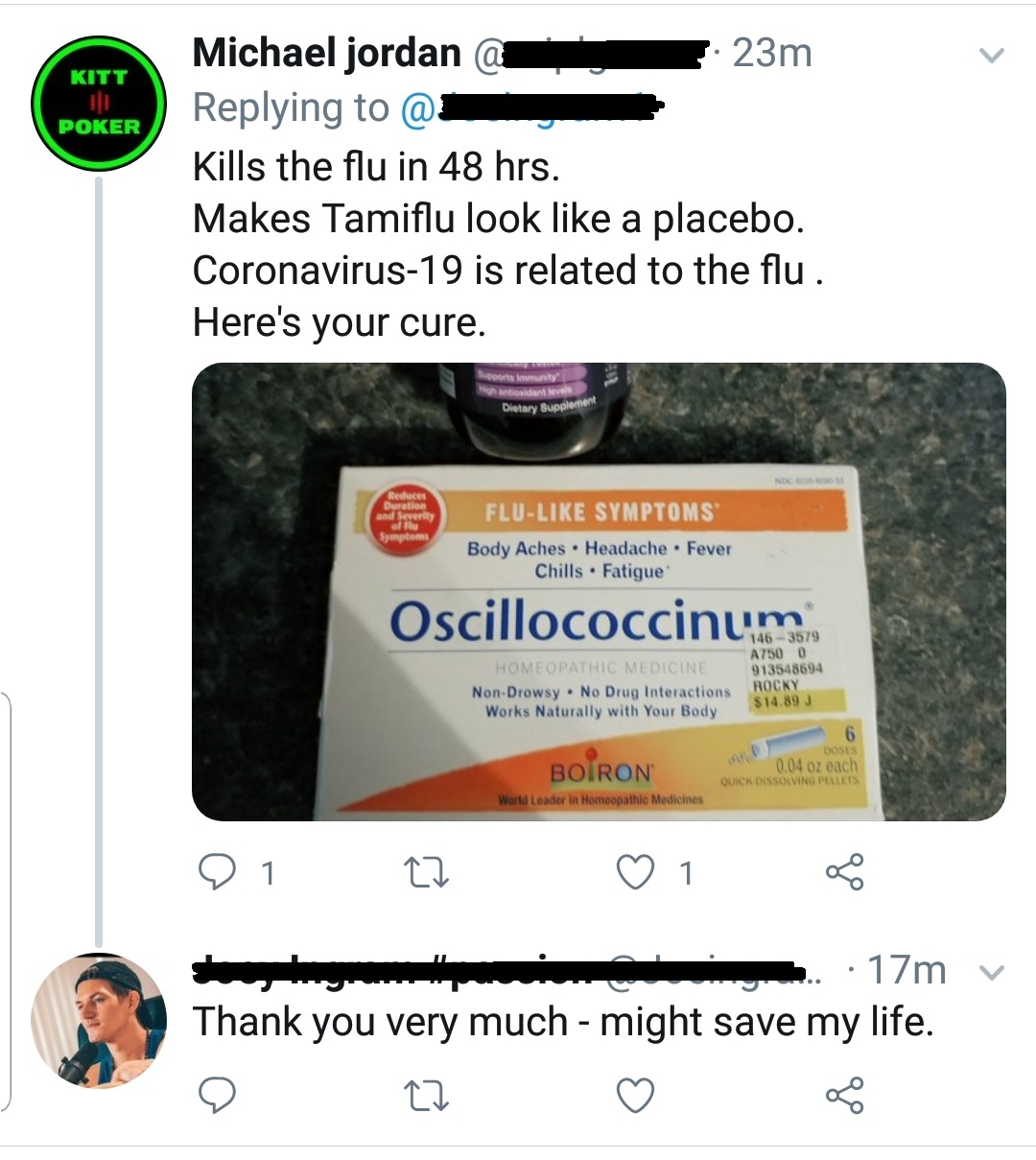
Does Tamiflu work on it? Right now – there’s no evidence for it, so this piece of information is pretty damn crap as there is no “placebo”. But oscillococcinum, though deceptive packaging (not to mention the confusing name) may suggest otherwise, is homeopathic, and thus, ineffective. Its development was based on the idea that influenza is caused by a strain of bacteria. It is not.
Vaccines and antivirals vs COVID-19
In terms of vaccines, the world is responding rapidly. I saw my doctor on March 6, 2020, and he informed me there were 2 phase 1 studies going on, already, for the coronavirus vaccine. While it may not be included in the flu shot for Australia this year, it almost definitely would by next year. Phase 1 studies are occurring around the world. This one is estimated to be completed by September 2020, this one will start recruiting soon, and this phase 1/2 study will be recruiting soon as well. Several antivirals, including remdesivir, which was developed to combat the ebola virus, are also undergoing clinical trials.
Will the flu shot save me from getting COVID-19?
Donald Trump was recently reported to have asked why the seasonal influenza vaccine couldn’t be used to stop coronavirus transmission. Vaccines are targeted towards activating your adaptive, target-specific immune system. Basically, this response by your immune system relies on training, and facilitating the spread and growth of killer cells and ‘antibodies’ that respond to a particular, disease specific target. So vaccines targeting certain strains of influenza won’t result in cells that kill the COVID-19 strain of coronavirus. But in having said that, my doctor recommended I get the flu shot to reduce my chances of getting the coronavirus, as doctors are in my local health district. Why? Because, through various mechanisms, such as the release of factors which suppress immune responses, or the killing of cells which normally would block infections from taking hold through various mechanisms too. This study modeled the potential for flu vaccines to prevent SARS outbreaks through the reduction of influenza in hospitals, where these diseases tend to spread most, and spread most severely. We know that the flu, likely most severe viruses for that matter, diminishes your immune system and makes you more susceptible to secondary infections. Though these are usually bacterial, it is very much possible, especially when there are numerous strains of diseases with very different genomic profiles (making it less likely T cells that may have developed in response to one infection could eliminate a secondary infection with another disease), as is the case with seasonal influenza and coronavirus coinciding, for viral infections to occur after having had another. So make sure you get your flu shot people!
Another curious issue is the name of the disease. Thus far, the disease itself has been named COVID-19, and the international Committee on Taxinomy of Viruses is calling the virus itself SARS-COV-2. The WHO and this committee put out their naming declaration on the same day. The only actually published announcement I could find on “SARS-COV-2” was in a non peer reviewed journal, making me feel some researchers wanted to jump the gun and get a name for it first, But considering the impact SARS had in Asia about a decade ago, the fear it entails, and the propensity for this to be blown out of proportion by media outlets, given the previous SARS epidemic had a much higher 9.4% mortality rate, the WHO recommends using COVID-19 when talking about this – which is what I’ve done throughout this piece.
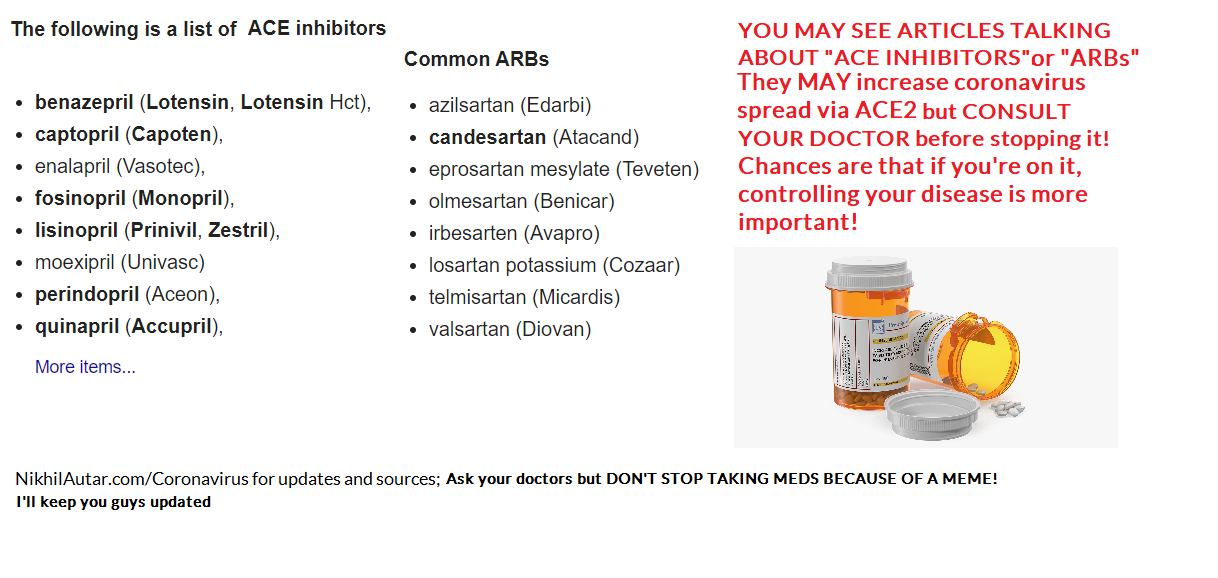
I saw something about ACE Inhibitors or ARBs (common heart drugs) being dangerous. Should I stop them?
But THIS IS JUST A STUDY and indeed a hypothesis for now. The study itself highlights the fact that there needs to be further investigation into this. Stopping ACE inhibitors and ARBs cold turkey will definitely make you feel crap and could possibly lead to more severe side effects or disease outcomes, depending on what you’re taking it for. So don’t do this
Is it a disease that only affects the elderly?
It’s true, as I outlined above, that elderly people do suffer most, and comprise the vast majority of deaths due to COVID-19. But not only is there a chance of young people dying to it too, as is being seen around the world, numbers from the CDC suggest that young people are not spared suffering. 12% of ICU patients are 20-44, 20% of people in hospital with it are in that age group too. 9% of deaths occur in the under 65 age group. None of this is insignificant. As I outline here, ICU is one of the most traumatizing things. And there are numerous reports of permanent lung fibrosis, or scarring, occurring too.
Can Children (and Anyone for that matter) get Permanent Lung Damage?
Early on in this virus, doctors were making claims that fibrosis was evidence in the lungs of patients with COVID-19. Fibrosis is a scarring element that is permanent.
These radiological findings have been confirmed, as seen in this medical journal of Australia review of sorts, which suggests up to 17% of severely ill, critical patients have evidence of fibrosis. A 15 year follow up of SARS coronavirus patients also confirmed that as many as 4.6% of a mostly healthy population had decreased lung function after their infection. Some health bodies are suggesting that this isn’t progressive fibrosis, which is good news in that it is not likely to cause long term inflammation in the lungs, but permanent disability and lung function is demonstrated through previous coronavirus outbreaks’ data, and through studies on radiological findings of the current pandemic – which suggests as many as 17% of severely ill patients are demonstrating signs of fibrosis (this number are likely to rise on follow up). It should also be mentioned that that Pulmonary Fibrosis Foundation is a press release, not a paper. It could be worse.
Children, though less likely to suffer from severe illness, are being admitted to ICUs in 0.58-2% of cases, according to CDC numbers in the US, and the most comprehensive study on paediatric outcomes out of China. It’s also evident that infants under 1 are at significantly higher risk of ICU admission (4x that of other children), and thus, exposure to this permanent damage. Not only is this linked to permanent lung damage, ICU admission causes severe trauma and PTSD too.
It is concerning to see that sending children back to school is being encouraged by governments around Australia, against medical consensus which suggests otherwise. Young people are similarly being asked to sacrifice themselves to attain herd immunity, but not only are there much higher rates of ICU admission and deaths being seen in 20-44 year old age groups when hospitals are overwhelmed, long term deleterious side effects of this through things like lung fibrosis is likely, and could have even worse economic outcomes in the long run too. Finally, sports leagues around the world, including our NRL, are also thinking about opening back up. With athletes in particular set to be severely impacted by lung damage, this should be taken into consideration too.
It’s not to say we shouldn’t reopen. But we should definitely not be looking to infect people to attain ‘herd immunity,’ not only because we’re not sure that proper forms of immunity will mount after infection (as opposed to vaccines which are optimized to create lasting infection – something I can explain further as a tumor immunology researcher), but because it could be much more dangerous than we imagine.
As someone who does have permanent lung damage of some kind due to chemo treatment, trust me, this is not something you want. I don’t know if I’ll ever be able to run again, yet alone do things like play basketball. You do NOT want this for your kids.
#DontRiskYourKids
What can you do to help?
Well the most effective organisation I could find, as judged by GiveWell and Charity Navigator (the number 1 and 2 evaluators of charities out there), is Direct Relief which is working with Chinese organisations and in the US and Carribean (and other places) to deliver money for research and PPE (personal protective equipment). That’s one way you can help.
Another way you can help is by Giving BLOOD! There is ALWAYS an outcry for more blood donations come influenza season, and blood banks around the world are doing the same.
Finally – the fact that there’s only been 1 study ever done on the impact of masks and hand hygiene on viral transmission rates globally irks me. My startup Centered Around You not only provides evidence based, AI powered wellness advice for the first time to general consumers, but also collects data in research friendly ways. Indeed, we have the potential to conduct a prospective follow up study, and more on this very task. Sign up for our email list to be kept aware of updates to this and to help aid research in this field.
And sign up to my email list to get updates on everything coronavirus and on other, mostly, health related stuff! I’m an ex cancer patient, current medical student, tumor vaccine researcher and founder of a few startups (to name a few things I do). I’d love to hear from you too! So check out my Facebook, YouTube, and Instagram if you’re there too!